Article Text

Abstract
Background This study aimed to determine the level of support for a sales ban on tobacco in England to provide a benchmark against which any changes over time can be assessed.
Methods 8735 people from England who participated in one of five monthly cross-sectional household surveys in 2008 were asked to indicate whether they would support the statement that ‘the government should work towards banning the sale of tobacco completely within the next 10 years’. In addition, sociodemographic and smoking characteristics were assessed.
Results A substantial proportion of the total sample (44.5%; 95% CI 43.5% to 45.6%) would support a move towards a complete ban. While never smokers (OR 2.02; 95% CI 1.82 to 2.25) and ex-smokers (OR 1.41; 95% CI 1.21 to 1.65) were more likely to support this idea, even among current smokers, a third would favour moving towards a sales ban of tobacco products. Adjusting for other background characteristics, younger, female participants, those living in London and those from lower socioeconomic groups were most likely to support a ban. Among smokers, a higher cigarette consumption, smoking enjoyment and contentment with being a smoker were associated with opposition to a ban, while feeling uncomfortable being a smoker, wanting to be a non-smoker and being worried about future health consequences of smoking were associated with support for a ban.
Conclusion Support for movement towards a ban on the sale of tobacco is higher than might be imagined. It is conceivable that as smoking prevalence falls further and smoking becomes more socially unacceptable, support might grow to a point where such a policy could become feasible.
- Advocacy
- end game
- public opinion polls
- public policy
- tobacco products
Statistics from Altmetric.com
Introduction
It would be inconceivable today to introduce a new drug to the market that would not only become addictive to its users but also kill them in the process. Yet, although tobacco products do exactly that, they are freely available for purchase by almost everyone. Put in its historical context, this anomaly arises from the rather lax attitude towards new consumer products at the turn of the 19th century, a time of little regulatory oversight which saw heroin marketed as an over-the-counter cough suppressant.1 Combined with a lack of knowledge about the health consequences and addictiveness of tobacco, and the introduction of industrial-scale cigarette production and persuasive advertising, this led to smoking becoming a mass phenomenon in the early 20th century.
At the height of cigarette consumption in the 1950s and 1960s, over half of the population in developed countries were smokers.2 At the same time, evidence for an association between lung cancer and smoking was beginning to accumulate3 4 and knowledge of the health hazards of smoking started to spread, culminating in the first US Surgeon General's report on the effects of smoking in 1964.5 This was followed by the introduction of health warnings on cigarette packs, restrictions on advertising and health promotion campaigns to educate people about the dangers of smoking, which resulted in a sharp drop in smoking prevalence throughout the 1970s, 1980s and 1990s in most developed countries.2 A further step was the introduction of comprehensive smoking bans, first mostly enacted in workplaces, but recently also extended to bars and restaurants in the UK and several other European countries, New Zealand, most of Australia and Canada and in many states of the USA, among others.6 There is little doubt that tobacco control measures have been effective in reducing smoking and while smoking prevalence is still at high levels in many developing countries,7 in many developed countries, such as Australia, Canada and Sweden, rates of smoking have now fallen below 20%.2
Given these positive changes over the last few decades in developed countries, a natural question to ask is where next? The state has at its disposal a continuum of controls—that is, government can apply absolutely no control, some regulation or total control in the production, distribution, communication and use of commodities. For instance, while there is some regulation on the production, distribution and communication of foodstuffs or energy, there is little control on their use. By contrast, little effective control exists on the production of illicit drugs, while their distribution, communication and use are under strongest legal controls.
With regard to tobacco, continuing with current successful control policies in terms of communication and use should further reduce prevalence and lead to denormalisation of smoking. Beyond that, one obvious choice is to regulate production more tightly—that is, to make cigarettes safer by removing toxins8 and/or to make cigarettes less addictive by removing nicotine.9 In conjunction with cigarette content regulation, other harm reduction strategies that encourage users to use safer (non-combustible) or clean pharmaceutical products have also been proposed.10 Moreover, regarding distribution of tobacco products, the transfer of the supply of tobacco from commercial corporations to non-profit enterprises has been suggested.11 This is to overcome the inherent problem that tobacco companies, by their very nature, aim to maximise profits through sales and can therefore not share in a meaningful public health mandate that seeks to reduce cigarette consumption.
Further down the line, even more extreme tobacco control measures may become feasible. An outright prohibition of smoking would present obvious challenges,12 and strong resistance is likely, even if it comes only from a minority. It has been argued that a ban would have adverse effects on national economies, but it has been demonstrated that in the long run there would probably be a net benefit.13 Public opposition is another alleged reason why tobacco has not been banned; yet, there is a surprising paucity of data to support this claim. In fact, evidence from the USA shows that nearly half of people would favour a complete ban.14 Once the level of opposition or support to such a policy has been established, it can be tracked, as was the case for smoke-free legislation,15 so that governments can decide on an appropriate timeframe to correct the anomaly. Given the lack of research in this area, the current paper examined the level of support in a representative population sample towards the most radical of tobacco control policies: a complete ban of the sale of tobacco. As such a drastic change in policy could obviously not be implemented immediately, the question was put in the context of a 10-year plan by the government to move towards banning the sale of tobacco completely.
Methods
Procedure and participants
The data were taken from the Smoking Toolkit Study, a series of monthly surveys designed to provide information on smoking behaviour and patterns among smokers and recent ex-smokers in England. The surveys are managed by the British Market Research Bureau and carried out using a random location sampling design described elsewhere (http://www.smokinginengland.info). Briefly, grouped output areas (containing 300 households) are initially randomly selected and stratified by ACORN characteristics (http://www.caci.co.uk/acorn/acornmap.asp) and region, followed by face-to-face computer-assisted interviews by trained interviewers with one member per household, and based on quotas which take into account the probability of being at home.
A total of 8735 respondents took part in five consecutive waves of the Smoking Toolkit Study carried out between August and December 2008, which included a policy question about moving towards a complete ban of the sale of tobacco.
Measures
Policy question
Respondents were asked to indicate whether they would support the statement that ‘the government should work towards banning the sale of tobacco completely within the next 10 years’ (Yes/No/Undecided). Those responding ‘no’ or ‘undecided’ were classified as not supporting a complete ban.
Sociodemographic characteristics
Data were collected on respondents' age, gender, social group (AB=higher and intermediate managerial/administrative/professional, C1=supervisory, clerical, junior managerial/administrative/professional, C2=skilled manual workers, D=semi-skilled and unskilled manual workers, E =on state benefit, unemployed, lowest grade workers) and place of residence (coded as London, South East, South West, East Anglia, East Midlands, West Midland, Yorkshire/Humberside, North West, North).
Smoking characteristics
Respondents were asked to indicate which best applied to them (Yes/No): (1) ‘I smoke cigarettes (including hand-rolled) every day’; (2) ‘I smoke cigarettes (including hand-rolled), but not every day’; (3) ‘I do not smoke cigarettes at all, but I do smoke tobacco of some kind (eg, pipe or cigar)’; (4) ‘I have stopped smoking completely in the last year’; (5) ‘I stopped smoking completely more than a year ago’; (6) ‘I have never been a smoker (ie, smoked for a year or more)’, (7) ‘Don't know’. Those responding ‘yes’ to (1), (2) or (3) were classified as current smokers. Respondents who said ‘yes’ to either (4) or (5) were classified as ex-smokers and those who responding ‘yes’ to (6) were categorised as never smokers.
Current smokers were further asked to indicate the number of cigarettes smoked per day and whether they had attempted to stop smoking in the last year. Current smokers were also asked to indicate whether they enjoyed smoking ‘very much’; ‘quite a bit’; ‘not particularly’; ‘not at all’; ‘don't know’, and how they felt about being a smoker (Yes/No): ‘I am happy with being a smoker; I am uncomfortable about being a smoker; I am worried that smoking is harming my health right now; I don't want to stop smoking but I feel I need to; I would love to be a non-smoker; I have had enough of being a smoker; I want to stop smoking; I ought to stop smoking; I intend to stop smoking soon; I intend to stop smoking but not soon; I am worried smoking will harm my health in the future; Don't know’. Smokers could indicate all that applied.
Analysis
Descriptive statistics were carried out to characterise the sample and provide prevalence data on attitudes towards tobacco policy. The sample was weighted to be representative of the English population. Simple associations between support for a total ban and sociodemographic and, if applicable, smoking characteristics were assessed with univariate logistic regression analysis. All variables were then included in a multivariate logistic regression to evaluate which, if any, of the assessed variables were independently associated with favouring a move towards a total ban of the sale of tobacco.
Results
The sample group had a mean age of 46 years (SD 18.7), 51.4% were female, 55.5% were in non-manual occupations and 22.3% self-classified as current smokers, 12.1% as ex-smokers and 65.5% as never smokers.
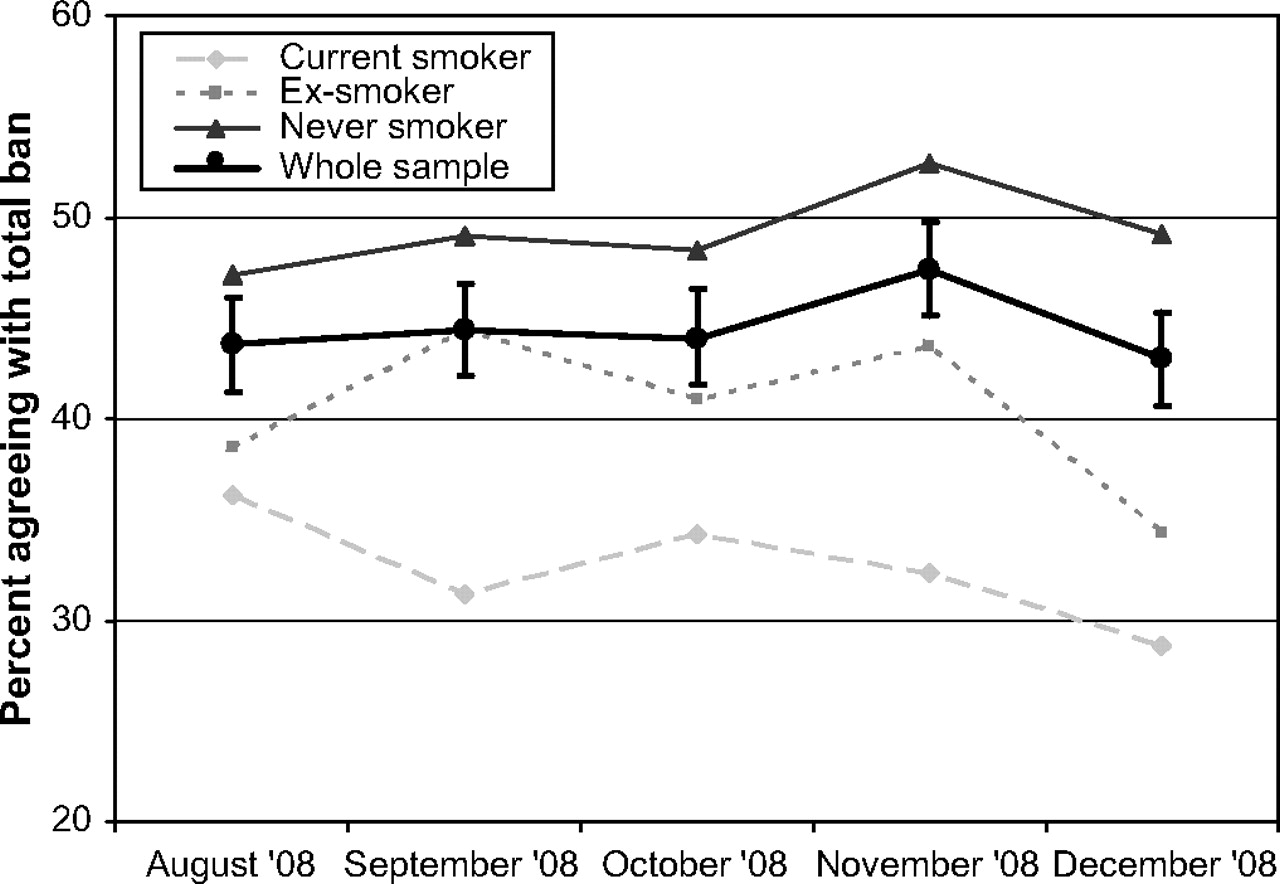
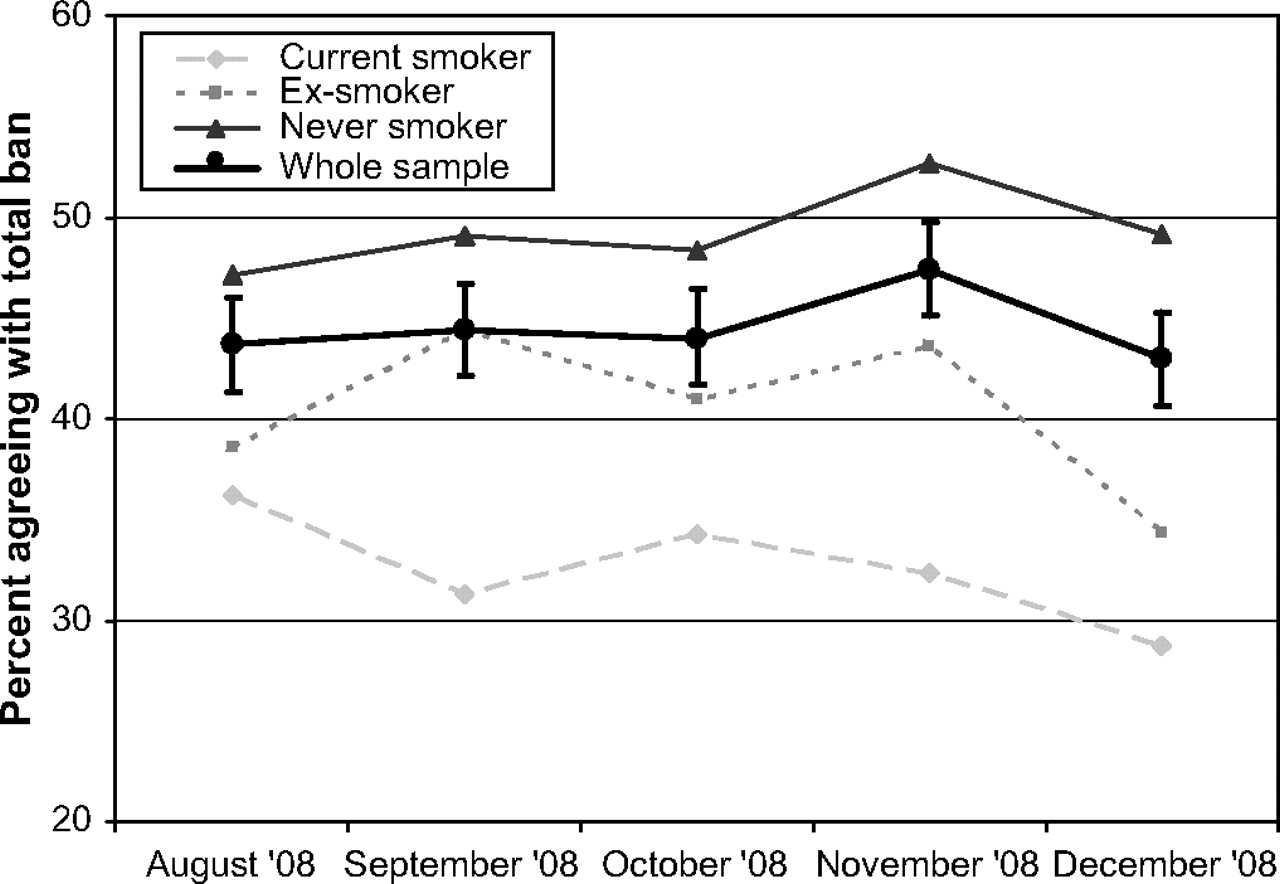
Opinion on moving towards banning the sale of tobacco was almost equally divided, and few respondents had no view on the matter. Although just over half were against a total ban (53.3%; 95% CI 52.2% to 54.3%), a considerable proportion (44.5%; 95% CI 43.5% to 45.6%) would support the statement that ‘the government should work towards banning the sale of tobacco completely within the next 10 years’; only 2.2% (95% CI 1.9% to 2.6%) did not express an opinion. There was no change in these rates across the five surveys (figure 1).
{kind=link}
Prevalence of support for a total ban on the sale of tobacco by smoking status.
Women were significantly more likely than men to support a total ban (47.0% and 41.9%, respectively; OR 1.23, 95% CI 1.13 to 1.34) and older respondents were less likely than younger respondents to support moving towards a ban of the sale of tobacco (per 10-year increment OR 0.77, 95% CI 0.69 to 0.85). While 47.6% of 16–24-year-olds would favour a ban, this figure was reduced to 40.9% in those above 65 years of age. No clear trend by social class was observed. However, Londoners were significantly more likely to support a ban on the sale of tobacco products than those in any other UK region (OR 1.75, 95% CI 1.45 to 2.12) and London was the only region where the majority (55.6%) was in favour of such policy. No interactions between smoking status or social grade and region were observed.
As expected, support for a total ban was dependent on smoking status; never smokers were more likely to be in favour of moving towards a ban than ex-smokers and current smokers (OR 1.44; 95% CI 1.26 to 1.64 and OR 2.02; 95% CI 1.82 to 2.25, respectively) and ex-smokers were more likely to support this policy than current smokers (OR 1.41; 95% CI 1.21 to 1.65). However, even among smokers a substantial minority (32.5%, 95% CI 30.4% to 34.6%) endorsed movement towards a complete ban on the sale of tobacco compared with 40.5% (95% CI 37.5% to 43.4%) of ex-smokers and 49.4% of never smokers (95% CI 48.1% to 50.7%).
When adjusting for other characteristics, the association between younger age and support remained (table 1). Women were more likely to approve a complete ban than men as were never smokers and ex-smokers compared with current smokers. Interestingly, after adjusting for other characteristics there was an inverse relation between social class and support with those in lower socioeconomic groups more likely to favour a sales ban. While support was homogeneous in most regions in the multivariate model, Londoners (followed by those in the North West) were far more likely to back a total ban on the sale of tobacco than any of the other regions in England (see table 1). There were no interactions between smoking status and any of the sociodemographic variables.
Multivariate association with support for a total ban on the sale of tobacco
We repeated analyses for the subsample of current smokers and included attitudinal as well as smoking characteristics in a multivariate regression model. Notably, there were no sociodemographic associations with support for a move towards a ban among smokers. However, a number of smoking and attitudinal characteristics emerged as predictive (table 1). Those who smoked more cigarettes per day, were happier being a smoker and enjoyed smoking more were less likely to endorse the proposed tobacco control measure. By contrast, feeling uncomfortable about being a smoker, wanting to be a non-smoker and being worried about future health consequences of smoking was positively associated with support for movement towards a ban of the sale of tobacco.
Discussion
While current tobacco policies have been effective in reducing smoking rates, tobacco use remains the main preventable cause of premature morbidity and mortality worldwide. Discussions and proposals on how tobacco control should evolve in the 21st century have continued.14 This study contributes to this debate by finding a substantial degree of support in the English population towards a move to ban the sale of tobacco completely. This level of support was relatively consistent over time, location and social class.
Even among current smokers, a third endorsed movement towards a ban. These figures compare favourably with pre-legislation support for the smoking ban in public places.16 While there were some regional differences, especially in London, suggesting that sociocultural characteristics may modify attitudes towards tobacco policy, responses were mostly homogeneous across other parts of England. The finding that younger people were more likely to favour a ban could indicate a less mature understanding of the implications of a sales ban of tobacco. However, in the context of falling youth smoking prevalence,17 this may equally signify a potential shift in attitude towards a tobacco-free environment among future generations. Respondents from lower social grades showed greater support. While one could speculate that this may reflect a greater willingness to accept state control or a different understanding of the consequences of changed legal treatment and potential public health benefits of a ban, it conflicts with the view sometimes advanced that more disadvantaged groups are less engaged with public health messages.18 Among smokers, it is interesting that sociodemographic characteristics did not appear to affect views on a ban. By contrast, the observed associations with potentially modifiable characteristics such as feelings about smoking suggest that targeted health promotion campaigns could increase support for a ban of tobacco products even among smokers.
It is obvious that outlawing the sale of tobacco is a highly contentious issue and would be difficult for any government to enforce.19 They first need to be assured of sufficient public approval and it is encouraging that these results demonstrate considerable support for this idea. However, as the experience in Bhutan shows,20 a workable solution needs to be in place in order for a ban to be successful. Indeed, the example of marijuana legalisation and delegalisation suggests that making an addictive product more easily accessible increases use,21 but complete prohibition does not necessarily decrease prevalence and may increase crime.22
What is a realistic way forward? First, current effective tobacco control measures need to continue in order to drive prevalence down even further. Smoking prevalence in the USA, for example, is predicted to fall to 14% by 2020.23 As smoking prevalence declines, so will its social acceptability, effectively denormalising the behaviour.24 Second, if smoking prevalence fell to sufficiently low levels—for instance, to that of regular illicit drug use (around 6% in England and Wales),25 this should pave the way for more radical policy changes and harm reduction strategies. Concurrently, non-combustible nicotine delivery devices and clean pharmaceutical products could be made available more easily (and possibly free of charge) to encourage long-term smokers to switch from cigarettes. Third, as stated in the introduction, such changes may require governments or non-profit organisations to purchase tobacco companies in order to remove resistance from cigarette manufacturers to regulatory impositions. Fourth, banning any substance from the free market is likely to increase smuggling and crime. For this reason, cigarettes will still need to be available for those smokers who cannot or do not want to stop. One suggestion would be to require smokers to have a prescription or licence to purchase cigarettes26 or to make cigarettes available only through healthcare providers. This model has shown promise in the treatment of opiate addicts who can receive methadone through the NHS.27 Lastly, no country exists in isolation and a coordinated global strategy on curtailing the supply of tobacco would need to be in place to avoid smokers freely accessing cigarettes abroad. While this is likely to present a significant problem, the ratification of the first worldwide public health treaty, the Framework Convention on Tobacco Control,28 by 168 countries provides some grounds for optimism that these hurdles may be overcome.
In this vision, by starting from a more acceptable de facto ban of the sale of combustible tobacco products,12 a de jure prohibition can be achieved at a later stage. The end result of denormalising smoking and removing cigarettes from public access would be a reduction of both uptake of smoking by adolescents and relapse rates among ex-smokers, eventually eradicating this most pervasive public health anathema of modern times.
This study has a number of limitations that restrict its generalisability. An obvious caveat is that the policy question was posed without providing a particular context as to how a total ban should be implemented. However, we did not aim to evaluate specific policy but rather were interested in the general attitude towards the idea of banning the sale of tobacco. When more detailed policies have been formulated, attitudes towards these can be gauged. Another issue relates to the stability and durability of findings. This study provides merely a snapshot of public opinion and views on this topic are likely to be fluid and may be different in the future. Indeed, in order to do justice to the enormity of the task involved, the question asked about moving towards a ban of the sale of tobacco in 10 years' time, and it may be that people are more willing to support a policy that is unlikely to be implemented in the near future. For this reason, it would be worthwhile to repeat surveys at regular intervals to assess changes in responses over time as a proposed ban becomes more probable.
Notwithstanding these limitations, the findings provide a first base for policy makers to better evaluate potential legislative changes and indicate that with an increasing denormalisation of smoking and introduction of novel harm reduction strategies, a real paradigm shift in tobacco control may be possible.
What this paper adds
Little is known about the attitudes in the general population towards future tobacco control policies.
This study finds a surprisingly high level of support for movement towards a complete ban of the sale of tobacco in England with younger, female non-smokers in London expressing the greatest level of support.
Acknowledgments
This study was funded by the charity Cancer Research UK, Pfizer, GlaxoSmithKline and Johnson and Johnson who had no involvement in the design of the study, the analysis or interpretation of the data, the writing of the report or the decision to submit the paper for publication.
References
Footnotes
Funding Cancer Research UK, Pfizer, GlaxoSmithKline, Johnson and Johnson.
Competing interests LS has received an honorarium for a talk and travel expenses from Pfizer. RW undertakes research and consultancy for the following developers and manufacturers of smoking cessation treatments; Pfizer, J7J, McNeil, GSK, Nabi, Novartis and Sanofi-Aventis. RW also has a share in the patent of a novel nicotine delivery device.
Provenance and peer review Not commissioned; externally peer reviewed.