Article Text

Abstract
Background Smoke-free legislation eliminating tobacco smoke in all indoor public places and workplaces is the international standard to protect all people from exposure to secondhand smoke. Uruguay was the first country in the Americas and the first middle-income country in the world to enact a comprehensive smoke-free national legislation in March 2006.
Objective To compare air nicotine concentrations measured in indoor public places and workplaces in Montevideo, Uruguay before (November 2002) and after (July 2007) the implementation of the national legislation.
Methods Air nicotine concentrations were measured for 7–14 days using the same protocol in schools, a hospital, a local government building, an airport and restaurants and bars. A total of 100 and 103 nicotine samples were available in 2002 and 2007, respectively.
Results Median (IQR) air nicotine concentrations in the study samples were 0.75 (0.2–1.54) μg/m3 in 2002 compared to 0.07 (0.0–0.20) μg/m3 in 2007. The overall nicotine reduction comparing locations sampled in 2007 to those sampled in 2002 was 91% (95% CI 85% to 94%) after adjustment for differences in room volume and ventilation. The greatest nicotine reduction was observed in schools (97% reduction), followed by the airport (94% reduction), the hospital (89% reduction), the local government building (86% reduction) and restaurants/bars (81% reduction).
Conclusion Exposure to secondhand smoke has decreased greatly in indoor public places and workplaces in Montevideo, Uruguay, after the implementation of a comprehensive national smoke-free legislation. These findings suggest that it is possible to successfully implement smoke-free legislations in low and middle-income countries.
- Tobacco smoke pollution
- nicotine
- secondhand smoke
- bars and restaurants
- smoke-free legislations
- environment
- environmental tobacco smoke
- public policy
- surveillance and monitoring
Statistics from Altmetric.com
- Tobacco smoke pollution
- nicotine
- secondhand smoke
- bars and restaurants
- smoke-free legislations
- environment
- environmental tobacco smoke
- public policy
- surveillance and monitoring
Introduction
Smoke-free legislation eliminating tobacco smoking in all public places is the international standard for the protection of all people, including workers, from exposure to tobacco smoke.1 Benefits of comprehensive smoke-free legislation include protecting non-smokers from the health consequences of secondhand smoke (SHS),2 3 motivating smokers to quit4 5 and reducing the number of people initiating smoking.6 Comprehensive smoke-free legislation, moreover, is easier to implement compared to incomplete smoking bans,1 7 causes no economic damage to the hospitality sector8 9 and is supported by most populations.10 11
In 2006, Uruguay was the first country in the Americas and the first middle-income country worldwide to enact a comprehensive smoke-free national legislation.12 Exposure to secondhand smoke in Uruguay before the legislation was very prevalent13 14 and protecting the population from SHS exposure in public places was urgently needed. The tobacco control movement began to form by the year 2000, as a coordinated effort between governmental sectors and civil society with the support of the Pan American Health Organization.15 16 After advocating for the signing and ratification of the WHO Framework Convention on Tobacco Control (FCTC), its major goal and success was the enactment of the comprehensive smoke-free legislation in March 2006 (Presidential Decree 268/05), reflecting in part the strong support of the president of Uruguay, Dr Tabaré Vazquez, a well known oncologist who made tobacco control a priority for the country. The presidential decree was confirmed as law on 10 March 2008 (Ley 18.256 Control del Tabaquismo).
To evaluate the impact of the 2006 comprehensive smoke-free legislation in reducing SHS exposure in Uruguay, we compared air nicotine concentrations measured in indoor public places and workplaces in Montevideo before (November 2002) and after (July 2007) the implementation of the legislation using the same study protocol during both study periods. Our goals were to track progress in reducing SHS exposure over time, to compare levels of enforcement across different locations and to identify potential needs for additional enforcement efforts.
Methods
Design and population
This study used passive samplers to monitor air nicotine concentrations in one hospital, two secondary schools, one local government building, one airport and 10 restaurants and bars using an established protocol.14 17a Sample locations were selected on a convenience basis to represent areas where people work or spend time. The hospital, schools, city government building and airport and eight restaurants and bars were the same in 2002 and in 2007. Two new restaurants and bars were recruited in 2007 to replace two establishments that no longer existed.
A total of 101 and 111 air samplers were deployed in 2002 and 2007, respectively. In 2002, one sampler located in a restaurant was damaged, leaving 100 samplers for analysis of air nicotine concentrations. In 2007, five samplers were lost in the hospital, one in the local government building and two in the airport, leaving 103 samplers for the analysis. Written and oral consent was obtained from the responsible authorities in each institution. The study protocol and consent forms were approved by the ethics review committees of the University of Uruguay, School of Medicine and the institutional review board of the Johns Hopkins Bloomberg School of Public Health.
Data collection
For each room where the sampler was placed, volume in cubic metres was estimated by measuring height, length and width with a tape measure and information on opening of windows and doors to outdoors and the use of mechanical ventilation systems was collected. During the 2002 sampling campaign we collected information on smoking policy (banned vs allowed). During the 2007 sampling campaign, we collected information on enforcement of the smoke-free legislation. We also added questions on cigarettes sales, and receiving tobacco advertisement and promotions from tobacco companies.
Nicotine monitoring
Air nicotine concentrations were estimated by passive sampling of vapour-phase nicotine.17b Samplers comprised a filter treated with sodium bisulfate, placed in 37-mm sampling cassette and covered with a porous diffusion membrane. Air nicotine samplers remained in bars and restaurants for 1 week and in all other locations for 2 weeks based on expected concentrations.14 Longer sample times provide improved analytical sensitivity by increasing the mass of nicotine collected. At the end of the sampling period, the samplers were securely closed and shipped to the Exposure Assessment Laboratory at the Johns Hopkins Bloomberg School of Public Health where the nicotine was extracted and analysed using gas chromatography with nitrogen-selective detection. The time-weighted concentration of air nicotine was estimated by dividing the amount of nicotine collected by the filter (μg) per volume of air sampled (m3). Volume sampled was calculated by multiplying the sampling time in each location by the effective sampling rate of the sampler (25 ml/min). For quality control purposes, 10% of samplers were duplicates and/or blanks. The intra-class correlation coefficient between duplicate samples was 0.98. Blanks were used to determine the blank-corrected nicotine concentrations and to calculate the nicotine limit of detection (0.003 μg/m3). In 2002, air nicotine concentrations were above the limit of detection in all samples. In 2007, seven samples collected in the schools had concentrations below the limit of detection. For samples below the limit of detection, a value of half the limit of detection was assigned.
Statistical analyses
Descriptive analyses were stratified by location and study year. To compare nicotine concentrations in the various locations by study year and other establishment characteristics we estimated the geometric mean and 95% CI of the air nicotine concentrations. Crude and room volume and ventilation-adjusted ratios (95% CIs) of geometric means of nicotine concentrations in 2007 versus 2002 were computed using linear regression models on log-transformed nicotine and entering study year as a dummy variable (2002=0 and 2007=1). These models allowed us to estimate the percentage reduction in nicotine concentrations as (1 − ratio)*100. The model also provided 95% CIs based on the corresponding CIs for the ratio. This analysis was conducted overall as well as stratified by institution and other characteristics. In sensitivity analyses we also ran the overall analysis using generalised estimating equations (GEE), with similar findings (results not shown). Analyses were conducted using Stata version 9.0 (Stata corporation).
Results
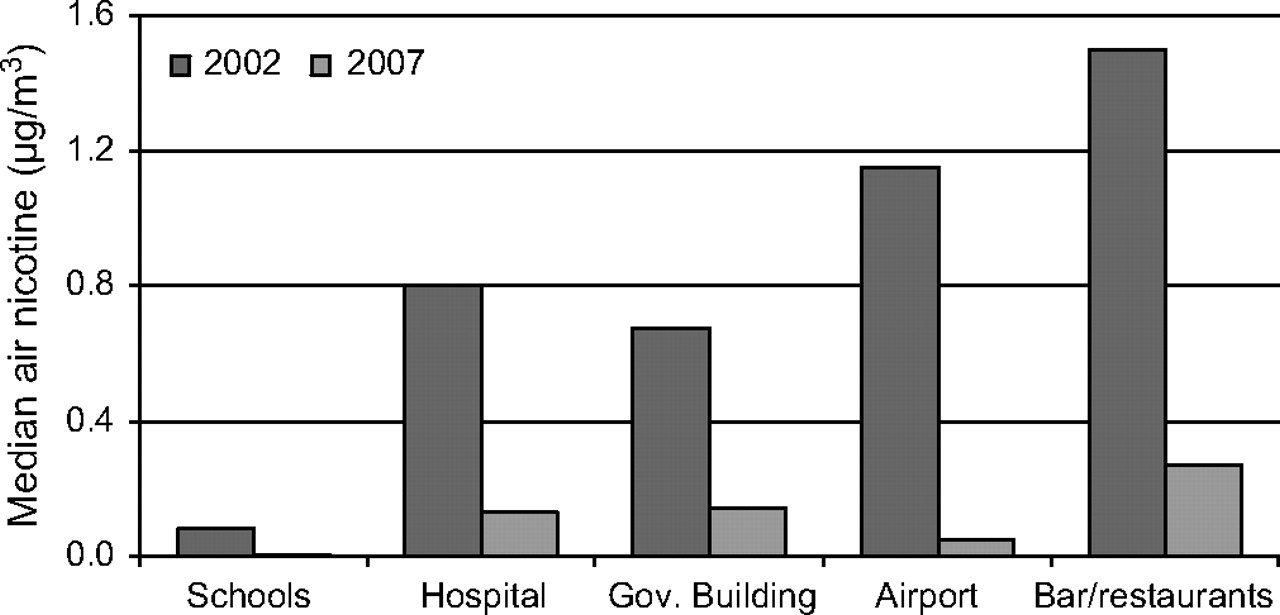
Median (IQR) air nicotine concentrations in the study sample were 0.75 (0.29–1.54) μg/m3 in 2002 compared to 0.07 (0.0–0.20) μg/m3 in 2007 (table 1). For both study periods, air nicotine concentrations were lowest in the schools and highest in the restaurants and bars. In 2007, smoking was not allowed in any indoor public place and workplace but in one restaurant, the owner indicated that employees smoked when the establishment was closed to the public. Air nicotine concentrations measured in 2007 in three bars/restaurants in which cigarettes were sold (median 0.43 μg/m3, IQR 0.27–0.86 μg/m3) and two bars/restaurants that received advertisements and promotions from the tobacco industry (median 1.54 μg/m3, IQR 1.06–2.21 μg/m3) were higher than the other bars/restaurants (median 0.23 μg/m3, IQR 0.09–0.30 μg/m3).
Number of samples and air nicotine concentrations in Uruguay, 2002 and 2007
Air nicotine concentrations changed markedly between 2002 and 2007 (table 1 and figure 1). The overall reduction in air nicotine concentrations comparing locations sampled in 2007 to those sampled in 2002 was 91% after adjustment for differences in room volume and ventilation. The greatest reduction was observed in schools. Excluding the restaurant where employees were allowed to smoke when the establishment was closed increased the adjusted reduction in air nicotine concentrations from 81% to 84% (95% CI 50% to 95%). Excluding the bars/restaurants that sold cigarettes and received advertisements and promotions from the tobacco industry increased it to 87% (95% CI 56% to 96%).
{kind=link}
Median air nicotine concentrations in public places in Montevideo, Uruguay, before and after the implementation of comprehensive smoke-free legislation in March 2006.
Discussion
Exposure to secondhand tobacco smoke has markedly decreased in indoor public places and workplaces in Montevideo, Uruguay, following the implementation of comprehensive national smoke-free legislation in 2006. Nicotine was practically eliminated in the air of the schools and the airport, reflecting high levels of enforcement of the legislation in these locations. In the hospital and in the city government building, nicotine concentrations were also very low, although somewhat higher compared to schools and the airport. In bars and restaurants, air nicotine concentrations measured in 2007 were lower compared to 2002, but remained higher compared to other locations, maybe reflecting contamination from outside smoking (allowed in contiguous open spaces belonging to these facilities), off-gased volatile smoke components from individuals carrying tobacco smoke components in their clothes or from heavy past exposure18 19 and incomplete legislation enforcement in some places.
Major reductions in secondhand smoke exposure have been shown in studies conducted in Ireland,20 Norway21 and Scotland22 before and after the implementation of comprehensive smoke-free legislations in these countries. The consistent findings in Uruguay support the feasibility of enacting and successfully implementing smoke-free legislations in countries other than high-income economies. Moreover, secondhand smoke reductions in Uruguay and in other countries implementing comprehensive smoke-free legislations20–22 have been greater than 75%, while in countries without legislation or with partial smoking ban legislations, no noticeable changes have been measured over time.23 24
In Uruguay, compliance with the legislation and popular acceptance has generally been high. Opinion polls conducted in 2006 and 2008 showed that more than 80% of the population approved it, including two-thirds of the smokers.25 Consistent with previous findings from other places, economic research conducted in Uruguay has shown no negative impact of the smoke-free legislation in the revenues of the hospitality sector.26 Protecting the population from the health consequences of secondhand smoke is the major goal of comprehensive smoke-free legislation. Growing evidence supports important reductions in acute coronary disease shortly after the implementation of smoke-free legislation.27–29 Decreased respiratory symptoms and improved lung function have been reported among bar and restaurant employees in California30 and Scotland.2 While similar benefits are expected in Uruguay, additional research is needed to evaluate the short-term and long-term health benefits related to the marked change in secondhand smoke exposure levels in public places in Uruguay.
Strengths of the study include the before and after design and the objective quantification of secondhand smoke using a specific marker of tobacco smoke.17b 31 While the sample locations were selected based on participation in 2002, the measures provide useful surveillance data regarding trends in secondhand smoke exposure levels in diverse indoor public places. The most likely explanation for the important reduction in air nicotine concentrations is the introduction of the smoke-free legislation in March 2006. However, we cannot ignore the possibility that seasonality differences or other unknown factors could account for part of the changes. Sampling locations were selected to represent locations where people frequently spend time but important locations also covered by the legislation such as universities, private workplaces or shopping malls were not included. Finally, while half of the population of Uruguay lives in Montevideo, information outside of Montevideo is lacking.
In summary, this before-after survey documents that exposure to secondhand smoke has greatly decreased in indoor public places and workplaces in Montevideo, Uruguay. Reduction of air nicotine concentrations following the 2006 comprehensive smoke-free legislation was above 80% in all locations and above 90% in the schools and the airport. In Uruguay, this success encourages the continuation of tobacco control efforts to reduce tobacco use and to protect the population from exposure to tobacco smoke in private places. For similar low and middle-income countries, the data from Uruguay represent a motivation to successfully implement smoke-free legislation.
What this paper adds
Secondhand smoke (SHS) exposure poses a serious risk for human health. In Uruguay, SHS exposure was widespread when smoking was allowed indoors.
This study found greatly reduced SHS exposure in public places and workplaces after the enactment of comprehensive smoke-free legislation in Uruguay.
The findings confirm comprehensive smoke-free legislation as a best practice to protect public health and represents a motivation to implement similar legislation in other countries.
Acknowledgments
We thank Mary Barros, Maria Laura Blanco and Gabriela Olivera for their important contributions to the fieldwork.
References
Footnotes
Funding Fligth Attendant Medical Research Institute (FAMRI).
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Ethical Review Committee of the University of Uruguay, School of Medicine Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health.
Provenance and peer review Not commissioned; externally peer reviewed.