Article Text

Abstract
Objective: To determine if there is a minimum duration, frequency or quantity of tobacco use required to develop symptoms of dependence.
Design and setting: A retrospective/prospective longitudinal study of the natural history of tobacco dependence employing individual interviews conducted three times annually in two urban school systems over 30 months. Detailed histories of tobacco use were obtained including dates, duration, frequency, quantity, patterns of use, types of tobacco, and symptoms of dependence.
Participants: A cohort of 679 seventh grade students (age 12–13 years).
Main outcome measures: The report of any of 11 symptoms of dependence.
Results: Among 332 subjects who had used tobacco, 40% reported symptoms, with a median latency from the onset of monthly smoking of 21 days for girls and 183 days for boys. The median frequency of use at the onset of symptoms was two cigarettes, one day per week. The report of one or more symptoms predicted continued smoking through the end of follow up (odds ratio (OR) 44, 95% confidence interval (CI) 17 to 114, p < 0.001).
Conclusions: Symptoms of tobacco dependence commonly develop rapidly after the onset of intermittent smoking, although individuals differ widely in this regard. Girls tend to develop symptoms faster. There does not appear to be a minimum nicotine dose or duration of use as a prerequisite for symptoms to appear. The development of a single symptom strongly predicted continued use, supporting the theory that the loss of autonomy over tobacco use begins with the first symptom of dependence.
- tobacco dependency
- youth
Statistics from Altmetric.com
Fundamental gaps exist in our understanding of the neurochemical and clinical manifestations of tobacco dependence. A variety of nicotinic acetylcholine receptor types are found in tissues ranging from neurons to white blood cells.1,2 Nicotine acts upon many different neurotransmitter systems in various areas of the brain, but how it causes dependence is unknown.1
Clinically, it is unclear which nicotine related symptoms represent neurochemical dependence and which represent nicotine's actions on other structures or physiological functions. For example, the American Psychiatric Association (APA) considers weight gain and a reduction in heart rate following the cessation of tobacco use to be manifestations of nicotine withdrawal and therefore, of dependence, but there is no evidence that these phenomena result from the same neurophysiological processes that produce dependence.3 While it is widely accepted that dependence has a psychological component, it is not known if psychological symptoms result from a pharmacological effect of nicotine, or arise through other mechanisms such as expectations, behavioural conditioning or associative learning.4 Until a role for nicotine is established for the psychological aspects of dependence, the term “tobacco dependence” may be more appropriate for use in clinical settings. Without an understanding of its pathophysiology, it has not been possible to develop a “gold standard” for identifying or measuring nicotine dependence.5
To provide a standardised nomenclature, official committees have issued a series of definitions of nicotine dependence.3,6,7 However, these are not mutually consistent, universally accepted, or derived from addiction theory.8–11 In most definitions, nicotine dependence is characterised by tolerance, craving, withdrawal symptoms, and loss of control over the amount or duration of use.3,4,6,7 Symptoms of nicotine withdrawal are said to include: craving, depressed mood, irritability, frustration, anger, anxiety, difficulty concentrating, restlessness, insomnia, headache, weight gain, and decreased heart rate.3,4,7,12–15
Even the core symptoms of nicotine dependence are debated. For example, the incentive–sensitisation model considers craving to be the central feature of dependence, but the APA has eliminated craving from its diagnostic criteria, while the World Health Organization has not.3,6,7,9,16 The validity of tolerance as a symptom of dependence is also disputed.11,16,17 Official definitions may reflect the prevailing opinion among committee members at the time, but do not represent a scientific gold standard.5,18,19 Additionally, the definition of nicotine dependence in the Diagnostic and statistical manual (DSM) defines when tobacco use qualifies as a mental disorder3; it does not establish when a smoker becomes “hooked”.
A recent exhaustive review of measures of nicotine dependence concluded: “the field lacks a widely accepted, theoretically derived, and psychometrically sound research tool for evaluating nicotine dependence.”8 With the lack of consensus over what constitutes nicotine dependence, there has been almost no published discussion of how its first manifestations can be identified, defined or measured.8
The criteria for diagnosing nicotine dependence as a mental disorder in adults may not be very useful for identifying emerging dependence in children. By analogy, histopathological criteria for the diagnosis of alcoholic cirrhosis would serve poorly as a tool to identify the earliest histologic signs of alcoholic hepatitis.
It is in this setting of controversy and uncertainty that the Development and Assessment of Nicotine Dependence in Youth (DANDY) study sought to explore how dependence begins. Conventional diagnostic criteria for nicotine dependence were not used in the DANDY study because we were interested in determining when the first symptoms of dependence appear and when youths lose their autonomy over their use of tobacco. The autonomy theory holds that dependence begins when full autonomy over tobacco use is lost—that is, when the sequelae of tobacco use, either physical or psychological, present a barrier to quitting.20 The appearance of any of the symptoms of dependence considered in this report indicates a loss of autonomy.20 The DANDY data strongly support the autonomy theory; the appearance of any single symptom of dependence was strongly predictive of failed cessation (odds ratio (OR) = 29) and continued smoking until the end of follow up (OR = 44), and was associated with daily smoking (OR = 58).20
The DANDY study addresses the question of when youths become hooked on tobacco; it does not address when youths meet the criteria for nicotine dependence as a mental disorder.3 The specific goals of the DANDY study were to determine: (1) the minimum time it takes adolescents to develop the first symptoms of dependence; (2) the minimum number of cigarettes that must be smoked each day before symptoms appear; (3) the minimum frequency of smoking below which symptoms do not occur; and (4) whether symptoms can precede the onset of daily smoking. There have been no prior studies of the onset of nicotine dependence. The literature on this topic is based on conjecture, or extrapolation from the observation of chronic smokers.21 For the past two decades, the onset of dependence has been conceptualised by the Stage Theory as a slow and sequential process, with the daily use of at least a half a pack of cigarettes as a prerequisite for dependence.3,4,21–27 Contradicting the Stage Theory, preliminary results from the DANDY study suggested that a rapid appearance of symptoms of dependence is common.28 This report presents results from the DANDY study after 30 months of prospective data collection.
METHODS
To study the onset of the first symptoms of dependence, a cohort of 679 seventh grade students (age 12–13 years) were enrolled in a longitudinal study. Starting in January 1998, subjects were interviewed individually in school three times each year over a period of three years. This report covers the first eight rounds of interviews.
The study was conducted in two small industrial cities in central Massachusetts with populations of 38 000 and 41 000 in 1990, and per capita incomes below the state average.29 These cities, with a combined service and industrial economic base, provide a rich mix of ethnic, cultural, and racial backgrounds. The study population was 68% non-Hispanic white, 20% Hispanic, 5% Asian, 4% African American;,0.6% Native American; and 2.5% unspecified. Among the white population, French and Italian ancestry were common. The socioeconomic status of the population covered the spectrum from poor to affluent.
There were 900 seventh grade students in the seven public schools in these two cities when the study began in January 1998. The following factors contributed to the selection of these cities: their large and ethnically diverse student bodies, the cooperation of the school administrations, and smoking rates comparable to the national average.30
As this is a descriptive study, the sample size was determined by a desire to produce reasonably precise estimates of all important descriptive statistics. Based on prior surveys, it was anticipated that 60% of subjects would try smoking and 30% would use it regularly. An assumed worst case attrition rate of 40% indicated an initial sample size of 650 was needed. With the approval of our institutional review board, the parents of all seventh graders were given the opportunity to withdraw their child from participating. Random number assignments were used to recruit 650 subjects. Prior tobacco use did not preclude participation. The initial 650 interviews were completed ahead of schedule allowing the sample size to be expanded to 679. Subjects were told the study concerned tobacco, and was confidential. This report covers the period January 1998 to June 2000.
A continuous record was maintained concerning demographic data, prior and current tobacco use, including the duration, frequency, amount, and pattern of use, the types of tobacco used, periods of abstinence, attempts to quit, and parental smoking status as reported by the subjects. The maximum rate of consumption was recorded and converted to units of days/year and cigarettes/year. Subjects were asked to provide exact dates for the first puff, inhalation, monthly use, and daily use, as well as the first occurrence of 11 symptoms of dependence (table 1).
Survey items concerning symptoms of dependence. The first 10 items constitute the Hooked On Nicotine checklist
A literature review located validated survey items used to identify dependence in previous studies.12,31–36 The 11 items listed in table 1 have been evaluated for their psychometric properties when used as a scale to measure the loss of autonomy over tobacco use.20,37 The item concerning sadness did not perform as well as the other 10 items, either in the DANDY study, or another by O'Loughlin and colleagues, but it was retained here as that was the initial study design.20,37 The autonomy theory of tobacco dependence states that the appearance of a single symptom of dependence indicates a loss of autonomy over tobacco use. As a test of the autonomy theory, the Hooked on Nicotine Checklist (HONC) was formed from the first 10 items in table 1.20 The HONC has an internal reliability of 0.94.20 A one factor solution explains 66% of the total variance. The number of HONC symptoms correlates with the maximum amount smoked (r = 0.65, p < 0.001), and the maximum frequency of smoking (r = 0.79, p < 0.001).20 Focus group testing has established that youths understand the HONC items in the same way as adults do.38
Structured interviews were conducted individually and privately in the schools three times annually. Four techniques proven to facilitate the accurate recall of dates and events were employed during interviews.39,40 These included the use of personal landmarks, bounded recall, decomposition, and a visual aide in the form of a personalised calendar.39,40 A calendar of significant events was created for each tobacco user and brought to each interview to serve as a memory aide and to assist in establishing the timing and sequence of events. Specific dates for smoking activities or symptoms were recorded when available. Otherwise, if an event was recalled to have occurred at the beginning of the month, it was recorded as the 7th of the month, the middle as the 15th, and the end of the month as the 25th.
Subjects who had used any form of tobacco were termed tobacco users and the date of first use was when a subject first puffed or used smokeless tobacco. A subject was termed a monthly smoker if he or she had ever smoked on two days within any 60 day period, representing a minimum frequency of use of one day per month. The onset of monthly smoking was taken as the date of the second day of smoking within the 60 day period. Thus, a subject who smoked his first two cigarettes on Monday and his third on Tuesday would be a monthly smoker on Tuesday, the second day of smoking, even though a month had not passed. All subjects who smoked on two or more days within any 60 day period (including daily smokers) would be monthly smokers. Tobacco dependence symptoms were operationally defined as follows: loss of control over the amount or duration of use as indicated by items 1 and 2 in table 1; an admission of feeling addicted to tobacco (item 3); craving or needing tobacco (items 4 and 5); difficulty controlling the behaviour as indicated by a positive response to item 6; or self report of any of the symptoms of nicotine withdrawal shown in table 1 (items 4, 7–11).
The first puff on a cigarette was before kindergarten for several subjects, and often, several years passed between the first and second cigarettes. The initiation of monthly smoking was thus judged to be a more meaningful baseline for measures of latency. The latency from the onset of monthly smoking to the first symptom of dependence was measured in days and is reported in completed 30 day months in the figures. If symptoms preceded monthly smoking, the latency had a negative value. Subjects with negative latency values, and those reporting symptoms within the first month, are graphed at a latency of zero completed months. For the question “Do you smoke now because it is really hard to quit?” the date recorded was the date of the interview, not the date when it first became hard to quit.
The Student's t test and the Mann-Whitney U test were used to compare means for normally distributed data and mean ranks for skewed data, respectively. Standard deviations (SD), standard errors (SE), odds ratios (OR), and 95% confidence intervals (CI) are reported. The χ2 was used to examine the relation between discrete variables. Logistic regression analysis and analysis of covariance were used to examine the role of sex as it was related to the number of symptoms of dependency while controlling for other factors such as age at first use or age at the time of monthly use.41 A probability value of p < 0.05 was used as a test of significance (NS, not significant).
RESULTS
Eight interviews were completed by 471 subjects (70%). The data presented include all 679 subjects in the initial cohort. The mean follow up was 728 days. The sample was 51% male, with a mean initial age of 13.1 years (range 12–15 years).
Prior use of tobacco was reported by 255 subjects (38%) at the first interview. Over the course of follow up, 332 (49%) had used some form of tobacco, 315 (47%) had puffed on a cigarette, 135 (20%) had puffed on a cigar, and 25 (4%) had tried spit tobacco. There were no regular users of cigars or spit tobacco.
Attrition rates did not differ by sex (females 32%, males 29%, χ2 = 0.44, NS). Attrition rates were higher for subjects who had a mother that had smoked (current smoker 39%, former smoker 29%, non-smoker 24%, χ2 = 13.4, p < 0.001), or a father who had smoked (current smoker 35%, former smoker 29%, non-smoker 22%, χ2 = 9.1, p < 0.01). Attrition rates were also higher for subjects that reported using tobacco before the first interview (38%) compared to subjects that had not smoked previously (26%, χ2 = 10.1, p < 0.005).
Our subjects were in the eighth grade during academic year 1998–99. By the middle of the school year, 38.4% had tried a cigarette and 6.6% reported daily use, compared to national figures of 44.1% and 8.1%, respectively.42 Tobacco use rates may have been lower than the national figures because of a greater attrition rate among our subjects that had used tobacco or were at higher risk for tobacco use because of parental smoking.
The mean age for the first use of tobacco was 11.7 years, and for the first monthly use 12.8 years. Inhaling on a cigarette was reported by 237 subjects (35%), with 145 (21% of the total population) progressing to monthly use, and 91 (13% of the total population) progressing to daily use. The mean latency from first use to daily use was 766 days with no significant sex differences (median 696 days, range 0–3601 days, SD = 751, n = 89). The mean latency from first use to monthly use was 486 days (median 158 days, range 0–3601 days, SD = 700, n = 144), and from monthly use to daily use, 251 days (median 70 days, range 0–1287 days, SD = 326, n = 89). Out of 332 subjects who had used any form of tobacco, when last interviewed, 75 (23%) were currently smoking, 54 (16%) had quit within the past three months, and 203 (61%) had quit for longer than three months.
Among the 332 subjects who had ever used tobacco, even just a puff, 132 (40%) reported symptoms of dependence, with a mean of 2.3 symptoms per subject (table 2). Among subjects who reported inhaling (n = 237), 53% reported symptoms, with a mean of 3.1 symptoms per subject (SD = 0.25). Strong cravings and needing a cigarette were the most commonly reported symptoms.
Cumulative symptoms of nicotine dependence among 332 young adolescents who had ever tried tobacco
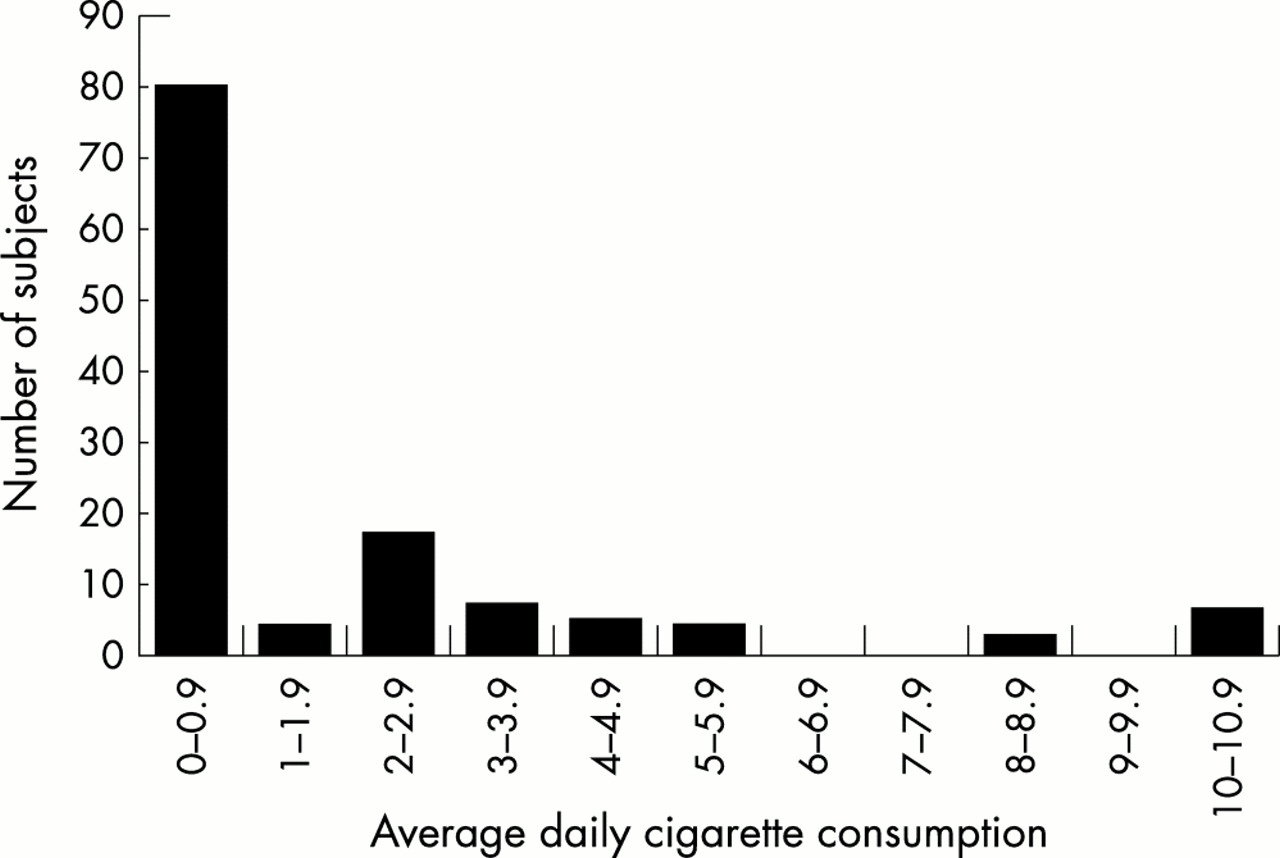
The frequency of use at the time of the first symptom was recorded for 125 subjects. Considering only subjects who had reported symptoms, 18% reported symptoms soon after their first use. Cumulatively, 33% reported symptoms when smoking at a rate of one day per month, 49% when smoking one day per week, and 70% before the onset of daily smoking (fig 1). The appearance that daily smoking is a significant milestone is an artefact of the ceiling effect inherent in measuring the smoking rate in units of days per week (fig 1). Many subjects who developed symptoms after initiating daily smoking did not do so until they were smoking several cigarettes per day (fig 2). In fig 2, it can be seen that the transition from smoking less than one cigarette per day to smoking one cigarette per day is not associated with a jump in the number of smokers reporting first symptoms. Nor is the smoking of a half pack per day (10 cigarettes). Ninety five per cent of symptomatic subjects reported symptoms before smoking a half pack per day. Out of 125 symptomatic subjects, a cumulative 52% reported symptoms by the time they were smoking an average of two cigarettes per week, and 65% by the time they averaged one cigarette per day. The mean level of consumption at the onset of symptoms was 583 cigarettes/year (SD = 945) with no significant sex differences. Parental smoking history was not significantly related to the frequency of smoking at the onset of symptoms. Taken together, the frequency and quantity data suggest that about half of the symptomatic youths had experienced symptoms by the time they were smoking two cigarettes in one day each week, and that about two thirds had symptoms by the time they were smoking one cigarette per day.

Average frequency of smoking at the time when the first symptom of dependence was experienced by 125 young adolescent smokers.
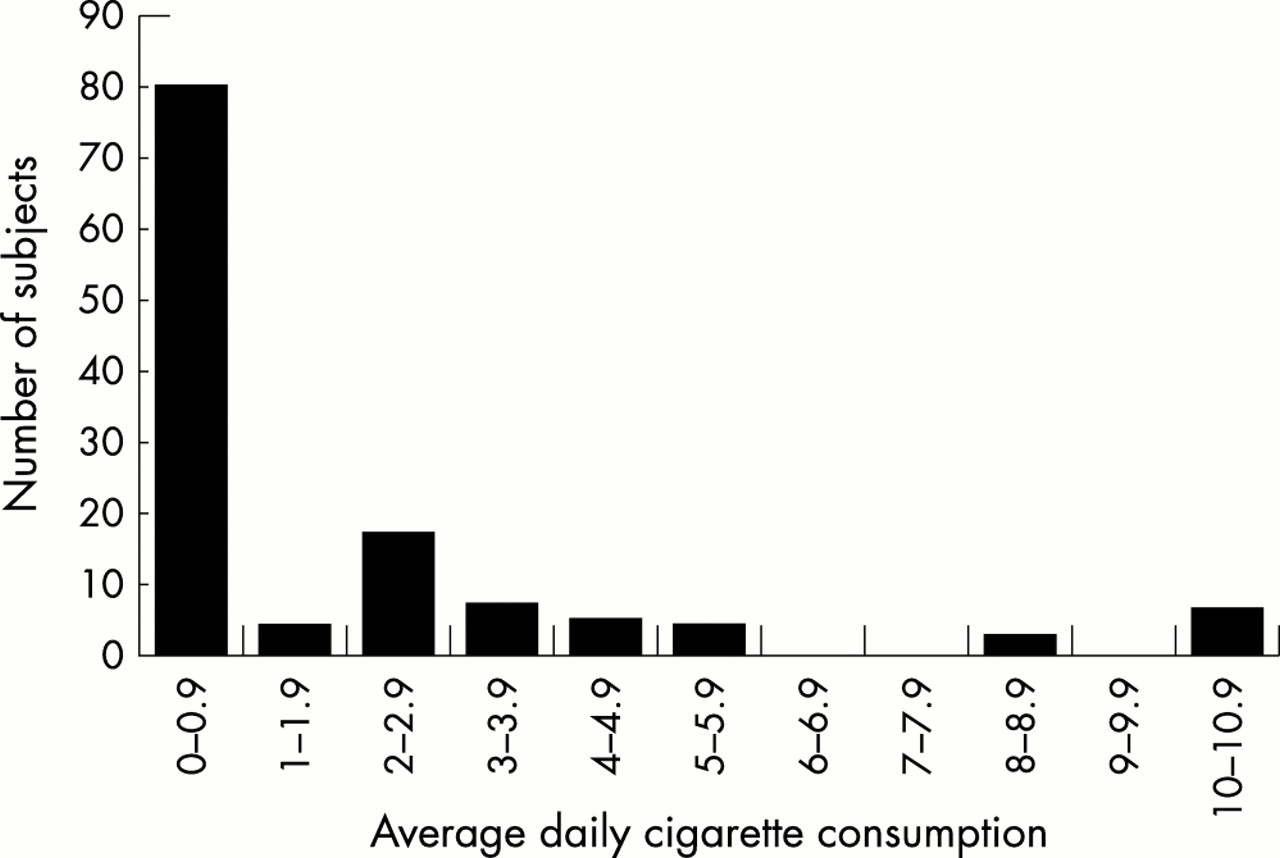
Average daily cigarette consumption reported at the time when the first symptom of nicotine dependence was experienced among 125 young adolescents.
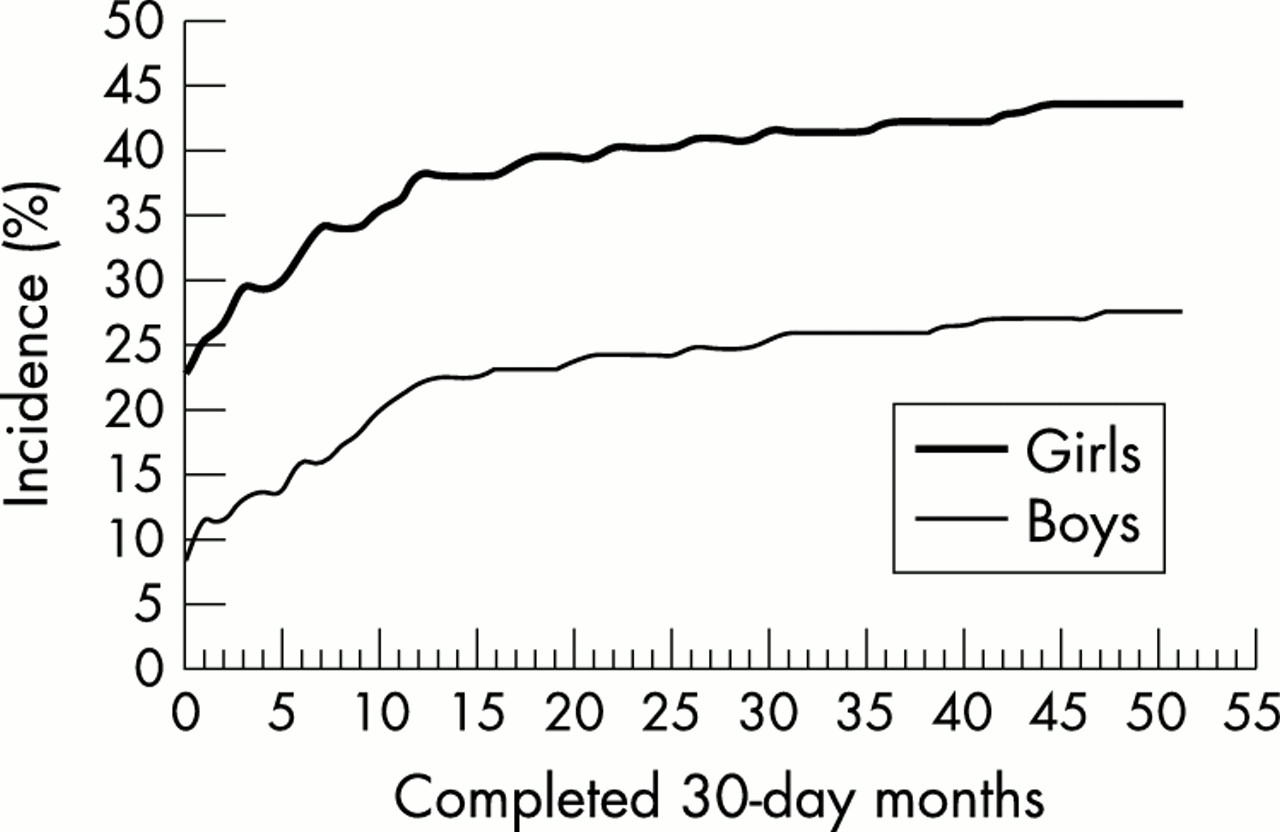
As depicted in fig 3, the time elapsed from the onset of monthly smoking to the first symptom was typically very short. Table 3 presents latency data for each of the 11 symptoms. It can be seen that the time course for the development of each of the symptoms is similar, indicating that the rapid onset of symptoms is not being driven by one, or a few symptoms. Subjects occasionally reported symptoms before smoking monthly. Latencies were calculated in terms of the number of days that had transpired from the onset of monthly smoking to the development of the first HONC symptom. The median latency was 54 days (mean (SD) 189 (427) days, range −1049 to 2025 days). As depicted in fig 4, girls reported a much faster onset of symptoms than did boys. Among subjects who reported symptoms, the median latency was 21 days for girls (mean 290 (448) days, range −609 to 2025 days) and 183 days for boys (mean 110 (396) days, range −1049 to 1329, Mann-Whitney U test, Z = −2.8, p < 0.005).
Latency period between the onset of monthly smoking and the appearance of the listed symptoms of dependence among 332 youths who had ever tried tobacco

Incidence of initial symptoms of nicotine dependence in 125 of 332 adolescents who had ever used tobacco according to the number of 30 day months completed from the onset of monthly smoking.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cumulative incidence of symptoms of nicotine dependence among 332 young adolescents who had ever used tobacco. Subjects who reported symptoms within the first month of tobacco use are plotted at zero completed months.
Significant sex differences were seen also in the number of symptoms reported (table 2). Each of the 11 symptoms was reported by a greater proportion of girls than boys, with the differences reaching significance for eight symptoms. Among all subjects who had tried tobacco, girls reported an average of 2.9 symptoms compared to 1.6 for boys (t = −3.31, p < 0.001). Among those who had progressed to monthly smoking, girls had a mean of 5.7 symptoms (SE = 0.43, 95% CI 4.9 to 6.6) compared to 4.0 for boys (SE = 0.44, 95% CI 3.1 to 4.9) after adjusting for age at the onset of monthly smoking using an analysis of covariance methodology (p < 0.05). There was no significant sex difference in the latency from first use to daily smoking (n = 89, mean 767 days, males 700 days, females 829 days, SD = 751, t = −0.81, p = 0.4).
An analysis was performed to determine whether a report of a single symptom was predictive of continued smoking until the end of follow up. Among 332 subjects who had ever used tobacco, those who, at any time during the study, had reported any of the 11 symptoms of dependence were more likely to have been current smokers at their last interview (OR = 44, 95% CI 17 to 114, χ2 = 116, p < 0.0001).
DISCUSSION
Symptoms of tobacco dependence were quite prevalent among this young population, with symptoms being reported by 40% of those who had tried tobacco and by 53% of youths who had inhaled. There did not appear to be any minimum frequency or amount of use required for symptoms to occur. Symptoms after a few exposures were common, confirming our preliminary report.28
The subjects in this study were not diagnosed as nicotine dependent based upon DSM criteria.3 We have proposed an alternative approach to assessing dependence, one that is derived from the autonomy theory.20 Our data suggests that the loss of autonomy in adolescents frequently occurs rapidly and at very low levels of nicotine exposure.28 The median consumption at the time of the first symptom was two cigarettes per week.
Symptoms of dependence apparently precede the development of chronic tolerance in most smokers. Before the development of chronic tolerance, smokers can satisfy their needs with only an intermittent cigarette and might feel little need to light up within five minutes of arising or smoke when sick in bed. Daily smoking and half pack per day smoking—behaviours which are clearly related to dependence in chronic adult smokers—showed no relation to the development of symptoms of dependence in our subjects.
The onset of symptoms has never been studied in adult onset smokers, so we are unable to comment on whether symptoms develop more quickly or at lower levels of consumption in adolescents or adults. But a significant body of evidence suggests that adolescents are more vulnerable to nicotine dependence. Brain development continues into adolescence, and perhaps because of this, the adolescent brain appears to be more vulnerable to nicotine.43–48 Individuals who begin smoking during adolescence are more likely to become dependent, to progress to daily smoking, to continue to smoke into adulthood, to smoke for a greater number of years, and to smoke more heavily as adults.25,49–53 Adolescents under 19 years of age are twice as likely to report difficulty quitting before smoking 100 cigarettes than are individuals of 19–22 years.31 Proven smoking cessation approaches have had disappointing results with adolescent smokers.54,55
The animal data also support a conclusion that adolescents are more vulnerable to nicotine. Nicotine infusions in rats result in the up-regulation of midbrain nicotinic acetylcholine receptor binding to a much greater extent in the adolescent than in the adult.56 Furthermore, this change is more persistent in the adolescent: one month into withdrawal, midbrain receptors are still significantly up-regulated in adolescents, but not in adults.56 In adolescent rats, nicotine induces cell damage in the hippocampus, and in both mice and rats, adolescents demonstrate greater impairment in reward system function after nicotine exposure.56–60 In parallel with the synaptic changes, nicotine has different, and sometimes opposite, behavioural effects in adolescent and adult animals.61,62
Together, the human and animal data suggest that juvenile onset nicotine dependence may differ in important ways from the dependence that results from exposing neurophysiologically mature individuals to nicotine. The current literature would support speculation that juvenile onset nicotine dependence may represent a more serious disruption of neurological functioning.56–59
It seems incredible that dependence might begin so quickly. What mechanisms might be operating? The calming effect of nicotine (thought to be mediated by the right hemisphere) is the primary reason given by adolescents for smoking.33,63–66 Some non-smoking youths appear to feel a need to self medicate symptoms of stress and turn to tobacco for this reason. If youths turn to tobacco to cope, it should not be surprising that some will develop an immediate psychological dependence. However, this cannot be the full explanation for the rapid onset of symptoms, since youths also quickly develop withdrawal symptoms that presumably indicate a physiological dependence. Animal experiments indicate that the neurochemical changes brought about by nicotine can develop quite rapidly. A dose of nicotine equivalent to a single cigarette produces long term potentiation of dopamine neurons in the ventral tegmental reward area, suggesting that the very first dose of nicotine “can leave its mark in the brain for a long time”.67
Nicotine causes an increase in the number of high affinity nicotinic cholinergic receptors in the brain structures associated with the reward pathway in both humans and rodents, an effect which is thought to play a role in addiction.2,68–74 The increase in receptor numbers parallels the development of tolerance, and receptor numbers decline after the drug is stopped, coinciding with withdrawal symptoms.68,71,74 Mice lacking the high affinity nicotinic cholinergic receptor will not self administer nicotine, suggesting that it is involved with the drug's rewarding properties.72 Nicotine infusions result in maximal up-regulation of receptors in just four days in mice, and in 10 days in rats.70,71 The up-regulation of nicotinic receptors has not been established as a mechanism causing nicotine dependence, but the rapidity with which these changes in brain structure develop makes it plausible that the first physiological symptoms of dependence might also appear quickly.
Consideration was given to possible methodological problems as an explanation for our results. To evaluate the possibility that repeated interviewing might result in prompting, the latency to symptoms was compared for subjects who reported symptoms at the first interview and for those who reported symptoms only after repeated interviews.28 There was no evidence that any significant prompting occurred; very short latencies were reported at the first interview.28
Many subjects reported the use of tobacco long before the first interview, opening the potential for recall bias. Analyses restricting the sample to subjects who developed symptoms after the study began did not alter the results.28 The short latencies cannot be attributed to postulated defects in individual survey items, since very short latencies were observed for all 11 survey items.28
The possibility that youths were reporting false symptoms as a result of prompting brought about by a desire to show off, a desire to please the interviewer, or expectations about nicotine dependence derived from sociocultural influences was considered. We have not found evidence of such expectations in adolescent focus groups (DiFranza JR, et al, unpublished data). These explanations are inconsistent with observations that the report of one or more symptoms was a strong predictor of failed cessation, continued smoking, and daily smoking, and are inconsistent with the observed correlations between the number of reported symptoms and the maximum amount and frequency of smoking.20 Expectations do not explain why youths experience difficulty quitting so soon after the onset of use since youths hold unrealistic expectations about the ease of quitting.48 Thus, we were unable to explain the observed results based on methodological problems.
What this paper adds
It has been widely assumed that moderate daily use of tobacco over an extended period of time is a prerequisite for nicotine dependence. The Development and Assessment of Nicotine Dependence in Youth (DANDY) study contradicts this view, with results indicating that the first symptoms of nicotine dependence can appear within a matter of days or weeks of the onset of intermittent tobacco use. These first symptoms were strongly predictive of long term tobacco use, indicating that the loss of autonomy over tobacco can occur very rapidly with minimal exposure to nicotine. The DANDY study has important implications for prevention strategies, cessation programmes, the measurement of nicotine dependence in youths, animal models of the neurobiology of nicotine dependence, and regulations intended to reduce the addiction potential of tobacco products.
Further support for the validity of the data comes from its consistency with previous studies reporting withdrawal symptoms among youths who were not smoking daily at the time of the interview, and a report that 8% of subjects who had smoked 20 or fewer cigarettes over their lifetime had difficulty quitting.12,31,32 These cross sectional studies were not subject to potential biases because of repeated interviewing.
In this study, girls reported more numerous symptoms of dependence and a much more rapid onset of symptoms. This was not caused by sex differences in attrition. Girls did not report more symptoms from their first inhalation such as dizziness or cough; there was no evidence that they over report symptoms generally.75 Sex differences in responses to nicotine in humans and animals have been recently reviewed.76 While some sex effects have been observed, they do not present a consistent pattern. At the lowest doses, female rats have acquired self administration of nicotine faster than males.77 Females were willing to lever press at higher rates than males to obtain nicotine, were quicker to earn their first dose of nicotine after a 23 hour period of deprivation, and displayed more pronounced sensitisation to the behavioural effects of nicotine.77 Using a modified version of the Fagerstrom Tolerance Questionnaire, Rojas and colleagues reported that male adolescents smoked more heavily and scored slightly more dependent than females, but they did not see any sex differences in the number of nicotine withdrawal symptoms or their frequency.78 Stanton reported that female adolescents were more likely to smoke to relieve withdrawal symptoms.79 Further study is needed to reconcile these differences and explore possible mechanisms.
The strengths of the DANDY study include a prospective design, a large diverse population (332 tobacco users, 237 inhalers), and an unselected sample evaluated in their natural environment over several years. Many studies of nicotine withdrawal symptoms among adults have been performed with only 20–50 highly selected subjects in laboratory settings.13–15,80 With its frequent follow up and use of memory aides to collect dates for events, this study is far more rigorous than any previously reported study concerning the timing of smoking events, some of which have required recall periods of 20 years or more.81,82
The higher attrition rate for subjects whose parents had smoked may have contributed to our inability to demonstrate any role of parental smoking in the onset of symptoms of dependence. The principal challenge to the interpretation of our results is the lack of consensus regarding what marks the onset of dependence. There is disagreement as to whether all of the items in table 1 are symptoms of dependence. All had been used as indicators of dependence, but in the absence of a gold standard for dependence, the validation of these items has typically been against some measure of nicotine intake or the ability to control use.12,31,34,47,83 The withdrawal items have been validated for adolescents against cotinine concentrations (a metabolite of nicotine).12 The item concerning smoking in forbidden places, adapted from the Fagerstrom Tolerance Questionnaire, also had been validated against cotinine concentrations.83 “Needing” tobacco has been widely cited as a symptom of dependence,12,33,35,36 and correlates very closely with the inability to control consumption.36 Craving as a manifestation of nicotine withdrawal has been documented in a laboratory setting.13,14 Absent another methodological flaw, it would be necessary to reject all 11 items in table 11 as symptoms of dependence to avoid the conclusion that symptoms develop quickly.28
Current criteria for nicotine dependence define the point when the use of tobacco represents a mental disorder.3 We feel that the loss of autonomy over tobacco represents a broader and more useful measure of the onset of dependence among adolescents. Youths can lose their autonomy over tobacco use—that is, they can get hooked, very quickly and at very low levels of nicotine exposure. Despite the rapidity with which the first symptom can appear, the presence of a single symptom of dependence strongly predicts that the initial attempt at cessation will be unsuccessful (OR = 29). An estimated 32% of all young smokers ultimately die prematurely as a result of their tobacco use.84 For some victims of tobacco, their unfortunate fates may have been cast with their first few cigarettes.

Making carcinogenic, addictive cigarettes is now an “art”, according to BAT Russia.
Acknowledgments
This study was funded by grant number CA77067–03 from the National Cancer Institute. The opinions expressed in this paper are those of the authors and do not necessarily represent the official views of the National Cancer Institute.