Article Text

Abstract
Objective: To examine the acute effects of AdvanceTM, a potential reduced exposure product (PREP) for smokers marketed as a means to reduce exposure to toxic gases and tobacco specific nitrosamines.
Design, setting, participants: Latin square ordered, three condition, laboratory based, crossover design with 20 smokers of light or ultra-light cigarettes (15 or more cigarettes/day). In each 2.5 hour condition, participants completed an 8-puff smoking bout from their own brand, AdvanceTM, or an unlit cigarette (that is, sham smoking) every 30 minutes for a total of four bouts.
Main outcome measures: Subject rated measures of tobacco/nicotine withdrawal; carbon monoxide (CO), and heart rate; plasma nicotine concentrations.
Results: Relative to own brand, AdvanceTM produced similar withdrawal suppression and heart rate increase, lower CO boost, and higher plasma nicotine concentrations.
Conclusions: PREPs for smokers need to be evaluated using a comprehensive strategy that includes empirical examination of acute and long term effects. Adequate withdrawal suppression and potentially lower concentrations of CO associated with AdvanceTM use are positive factors, although higher nicotine concentrations do not constitute “reduced exposure”. Overall, longer exposure periods are necessary to determine carcinogen delivery. PREP evaluation is complex and should be completed objectively.
- AdvanceTM
- potential reduced exposure product
- CO, carbon monoxide
- HR, heart rate
- HSD, honestly significant difference
- IPI, interpuff interval
- NS, non-significant
- PREP, potential reduced exposure product
- QSU, questionnaire of smoking urges
- TSNs, tobacco specific nitrosamines
- VAS, visual analogue scale
Statistics from Altmetric.com
- CO, carbon monoxide
- HR, heart rate
- HSD, honestly significant difference
- IPI, interpuff interval
- NS, non-significant
- PREP, potential reduced exposure product
- QSU, questionnaire of smoking urges
- TSNs, tobacco specific nitrosamines
- VAS, visual analogue scale
The causal relation between tobacco smoking and premature death is well documented1 and is attributable to hundreds of tobacco smoke delivered toxicants, including carbon monoxide (CO)2 and tobacco specific nitrosamines (TSNs).3 Despite wanting to avoid these toxicants, most smokers find quitting difficult because they are dependent upon cigarette delivered nicotine.4 The tobacco industry may have hoped to reduce inhaled toxicant levels with “low yield” cigarettes that seemed to deliver lower concentrations of nicotine, CO, and other toxicants (“tar”). However, after decades of use in the USA, these products did not reduce tobacco associated mortality.5 Regrettably, when these products were introduced, little information describing their potential risks was available to smokers. In retrospect, demonstrations that “low yield” and regular cigarettes deliver similar toxicant levels may have led more smokers to quit rather than switch to the new products.6
In the USA, the industry has recently released new potential reduced exposure products (PREPs—for example, Eclipse®, AdvanceTM) that may be intended to reduce inhaled toxicant levels. Policymakers and smokers need to know the risks associated with these products, but there have been few objective pre-marketing evaluations of them. Objective post-marketing evaluation, in the form of acute exposure studies, reveals important characteristics of some PREPs, such as Eclipse®’s greater-than-usual-brand CO delivery.7 Like Eclipse®, AdvanceTM purportedly reduces toxicant levels (that is, TSNs and “toxic gases”; AdvanceTM package “onsert”). There are no objective studies that describe this PREP’s effects in smokers. While several days’ exposure is required for any measurable difference in TSN delivery to be observed (TSN metabolites have a distribution half life of 3–4 days8), acute studies can help to determine other PREP effects. This acute study examines how exposure to AdvanceTM cigarettes influences nicotine and CO delivery, heart rate, and tobacco/nicotine withdrawal symptoms in smokers; TSN exposure is not a focus of this acute study.
DESIGN
Participants and setting
Advertisements were used to recruit 10 women (2 non-white) and 10 men who completed this institutional review board approved, three condition, Latin square ordered, within subjects study. Individuals were included if they were 18–50 years old (mean (SD) 25.8 (6.0)), provided a breath sample ≥ 15 parts per million (ppm) CO at screening (mean 25.1 (9.2)), and smoked ≥ 15 king sized, non-mentholated, “light” or “ultra-light” cigarettes/day (mean 20.7 (4.7)). Participants were moderately nicotine dependent, as indicated by the Fagerstrom9 nicotine tolerance questionnaire (mean 5.3 (1.6)). Exclusion criteria included previous AdvanceTM experience, past or current cardiovascular disorders and current pregnancy, breastfeeding, or smoking cessation or reduction efforts. All participants provided written, informed consent before and were paid $200 after participation.
Materials
Opaque tape was used on all own brand (Own) and AdvanceTM (Adv) cigarettes throughout the study to blind participants (but not experimenters) to cigarette condition and to cover 100% of filter vent holes (approximately 57% of smokers cover vent holes with their fingers or lips10). By the Federal Trade Commission (FTC) method11 (in which vent holes are not covered), on average, Own yielded 0.73 mg nicotine, 10.7 mg CO, and 9.4 mg tar; Adv yielded 0.8 mg nicotine, 9.1 mg CO, and 9.8 mg tar.
Main outcome measures
Computerised visual analogue scales (VAS) consisted of an item above a horizontal line that had anchors on the left (“not at all”) and right (“extremely”). Subjects moved a mouse controlled cursor and clicked to produce a vertical mark on the horizontal line. The score was the distance of the vertical mark from the left anchor, expressed as a percentage of line length. VAS items12 described tobacco/nicotine withdrawal symptoms: “Urges to smoke”, “Irritability/Frustration/Anger”, “Anxious”, “Difficulty concentrating”, “Restlessness”, “Hunger”, “Impatient”, “CRAVING a cigarette/Nicotine”, “Drowsiness”, “Depression/Feeling blue”, and “Desire for sweets”. Another subjective effect measure, the 32 item questionnaire of smoking urges (QSU), yields two empirically derived factors: factor 1 (intention to smoke) and factor 2 (anticipation of relief from withdrawal).13
For puff topography, cigarettes were smoked through a mouthpiece connected to a pressure transducer, and pressure changes were amplified and digitised. Software (Plowshare Technologies, Baltimore, Maryland, USA) converted signals to airflow (ml/s) and integrated the data over time for each puff, producing measures of puff volume, duration, and interpuff interval (IPI).
Heart rate (HR) was monitored continuously (Monitor 507E, Criticare Systems, Waukesha, Wisconsin, USA) and recorded every 20 seconds. CO was measured before and, on average, 5.1 (0.5) minutes after each cigarette (BreathCO, Vitalograph, Lenaxa, Kansas, USA). To measure nicotine delivery, blood samples were centrifuged and the plasma removed and stored at −70°C. Samples were analysed using gas chromatography/mass spectrometry.14
Procedure
Cigarette abstinence (that is, CO concentration of ≤ 10 ppm) was required before each of three approximately 2.5 hour conditions. Conditions were separated by at least 24 hours, and were defined by whether the subjects puffed from lit Own, lit Adv, or unlit cigarettes (Sham15). Experimental sessions began with blood sampling (10 ml; forearm venepuncture). Next, continuous recording of HR commenced. After 30 minutes, the first of four smoking bouts began; all bouts were separated by 30 minutes and consisted of pre-smoking CO and subjective effect measurement, eight self paced puffs, and post-smoking subjective effect and CO measurement. The session ended with blood sampling, on average 12.8 (4.7) minutes after the last puff.
Data analysis
HR data were averaged to produce one value for each of four pre-smoking (10 minutes before smoking) and smoking periods.15 Topography data (n = 18, data from two participants were lost because of computer/administrative error) were treated as in previous work,7,16 and data for each of the four cigarettes were averaged for each subject using all remaining values for puff volume, duration, and IPI. For the plasma nicotine analysis, values below the limit of quantification (1.0 ng/ml) were replaced with a value of 1.0 ng/ml.
Data were entered into a within subjects analysis of variance with three factors: condition, smoking bout (except for plasma nicotine data), and time (except for topography data). Significance levels were adjusted for violations of the sphericity assumption using Huynh-Feldt corrections; Tukey’s honestly significant difference (HSD) was used to examine differences among means.
RESULTS
Significant condition by bout by time [C*B*T: Fs (6,114) > 2.8, p < 0.05] or condition by time [C*T: Fs (2,38) > 4.1, p < 0.05] interactions were observed for all subjective measures except the “Depression/Feeling blue” VAS. Scores on subjective measures were high before the first smoking bout and decreased similarly after each bout in Own and Adv conditions. For example, on the “CRAVING a cigarette/Nicotine” VAS, mean (SD) scores for the first bout decreased from 72.0 (33.2) to 26.1 (27.7) in the Own condition and from 68.9 (33.6) to 21.1 (25.3) in the Adv condition (p < 0.05). Mean scores increased from 66.6 (38.3) to 67.8 (36.6) in the Sham condition (NS). By the end of the fourth bout, mean scores had decreased to 16.7 (27.7) for Own and 16.5 (25.6) for Adv, but were 74.1 (36.0) for Sham. This pattern of results was similar for other subjective measures. For topography, a condition main effect [F(2,34) = 22.3, p < 0.001] was observed for IPI, with shorter IPIs (p < 0.05) for Sham (mean 17.2 (14.2) s), relative to Own (33.9 (23.6) s) or Adv (34.5 (21.9) s). Condition did not influence puff volume (Sham 66.5 (43.7) ml; Own (56.5 (11.2) ml; Adv 51.6 (9.4) ml) or duration (Sham (2.1 (1.0) s; Own 1.8 (0.1) s; Adv (1.8 (0.1) s).
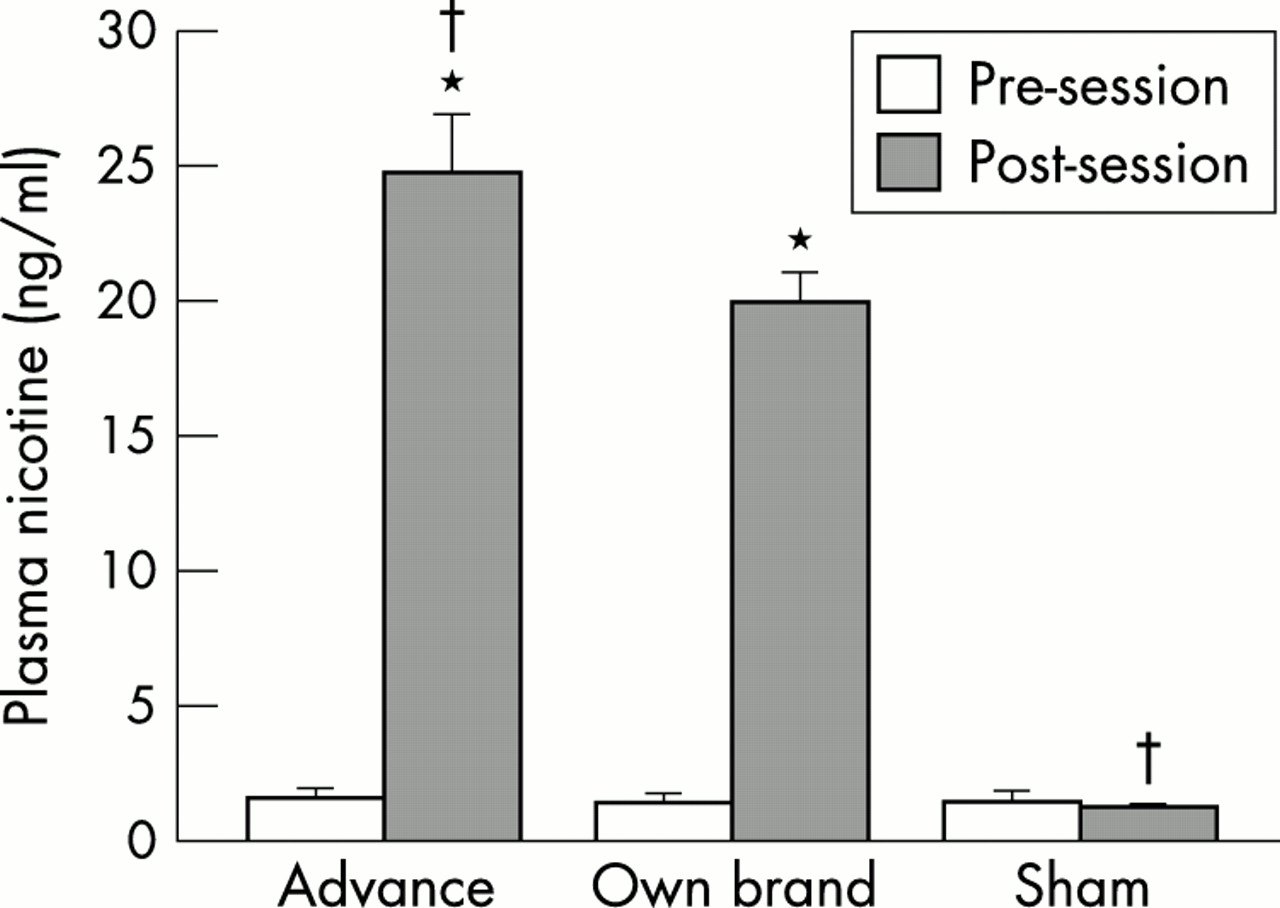
Condition influenced HR [C*B*T: F(6,114) = 10.6], CO [C*T: F(2,38) = 162.3], and plasma nicotine [C*T: F(2,36) = 133.4] (p < 0.001). Mean (SD) HR in the first bout increased from 69.8 (7.3) to 80.7 (7.7) beats/min for Own, from 70.3 (9.8) to 83.2 (11.9) beats/min for Adv (p < 0.05), and from 69.3 (8.5) to 70.5 (10.2) beats/min for Sham (NS). During the fourth bout, mean HR was 76.2 (8.3) beats/min for Own and 77.2 (10.4) beats/min for Adv, but had decreased to 66.9 (9.6) beats/min for Sham. Mean CO in the first bout increased from 6.4 (2.0) to 12.4 (3.1) ppm for Own, from 6.5 (2.9) to 12.2 (3.6) ppm for Adv (p < 0.05), but had decreased from 6.9 (2.3) to 6.6 (2.3) ppm for Sham (NS). By the end of the fourth bout, mean CO was 25.4 (6.1) ppm for Own, significantly greater than the 23.4 (5.9) ppm for Adv and 5.7 (2.0) ppm for Sham (p < 0.05). As shown in fig 1, plasma nicotine concentrations increased by 23.3 ng/ml for Adv, significantly greater than for Own (18.6 ng/ml) and Sham (−0.2 ng/ml; p < 0.05).

{kind=link}
Averaged data (plus one SEM) from 20 subjects for plasma nicotine concentration for AdvanceTM, Own brand, or Sham. Open bars are data collected before each session; filled bars are data collected after each session. *Significant pre-post session difference; †significant difference from Own brand at that time point (all p < 0.05, Tukey’s HSD).
DISCUSSION
Acute exposure using clinical laboratory methods has proven value in the evaluation of PREPs for smokers7,12,17; this study is the first published work to examine this particular PREP using this methodology. In the current acute study, relative to own brand cigarettes, AdvanceTM suppressed withdrawal fully, while delivering 11% less CO and 25% more nicotine. Differences in CO and nicotine delivery may reflect AdvanceTM tobacco content and/or filter design, but cannot be explained by changes in smoking topography. No compensatory changes in topography were observed with AdvanceTM, despite the fact that the acute exposure methods used are demonstrably sensitive to topography changes (for example, when smokers switch from unventilated to ventilated cigarettes,18 or from regularly marketed cigarettes to PREPs12,17). CO and nicotine delivery results may also reflect the fact that filter vent holes were blocked in all cigarettes used in this study (that is, tape occluded 100% of the vent holes on own brand and Advance™ cigarettes). Further research will reveal if unblocked filter vent holes produce differential puff topography values (for example, larger or smaller puffs, more or fewer puffs) with corresponding changes in CO and nicotine delivery of Advance™ cigarettes. The presence of filter vents, and the uncertainty regarding who blocks them and how many are blocked, highlights the complexity of PREP evaluation, and suggests that PREPs with filter vents may need to be tested with and without vent blocking, using the clinical laboratory methods outlined here and elsewhere.7,12,17
The 11% reduction in CO and 25% increase in nicotine delivery may or may not influence smoking’s health risks. CO contributes to a variety of smoking related disease, so any meaningful reductions should be encouraged; other PREPs completely decrease CO delivery.12,17 Increased nicotine delivery may decrease smoke exposure if smokers use fewer cigarettes and/or take fewer or smaller puffs. Conversely, a cigarette that delivers higher than usual nicotine concentrations may increase nicotine dependence level, if smokers do not alter their smoking topography. In acute studies when non-treatment seeking smokers received 100–200% of their usual daily nicotine dose,19,20 the number of cigarettes smoked did not decrease significantly, though some decrease in smoke delivered nicotine (25–40%) was observed, presumably due to compensatory reductions in cigarette smoke intake. The issue of longer term changes in smoking behaviour in response to AdvanceTM (that is, increased or decreased puff volume as a result of greater nicotine delivery), as well as the potential for reduced TSN delivery, awaits longer term exposure studies.
Understanding the risks associated with widespread PREP use requires careful, objective evaluation.7,21 One evaluative approach, apparently endorsed by the tobacco industry, is to test market PREPs for smokers in an unregulated manner that includes no clear assessment methods. In the past, a similar approach led to widespread belief that “low yield” cigarettes reduced the health risks of smoking when, in fact, these products failed to reduce tobacco associated mortality.5 Another evaluative approach might involve acute and longer term studies of PREPs that are carried out before the products are marketed, under strict regulatory oversight, and with clear assessment methods. Once implemented, this pre-marketing, regulated evaluative approach may help to predict whether or not PREP use is likely to be associated with a reduction in any of the myriad health risks that smokers face. It will also likely reveal if PREPs introduce new risks not currently associated with cigarette use (for example, inhaled glass fibres22). The current results, along with similar evaluations7,12,17 and past experience, make clear that PREP evaluation is complex, and should not be left in the hands of an industry that profits handsomely from PREP acceptance and use.
Acknowledgments
This work was supported by USPHS grants DA 11082, DA 06052, DA 07027, and MO1-RR00065, as well as the Robert Wood Johnson Foundation’s Tobacco Etiology Research Network. Portions of this work were presented at the Eighth Annual Meeting of the Society for Research on Nicotine and Tobacco, 20–23 February 2002.