Article Text

Abstract
Objective: This study seeks to determine the magnitude, nature, and correlates of social exchange of cigarettes among youth who smoke.
Design: Cross sectional survey.
Setting: Schools in 29 Minnesota communities.
Participants: All students in grades 8, 9, and 10 (ages 13–16 years) in each participating school. The parent/child response rate for the survey was 90%. Analyses included 4124 respondents who smoked at least one cigarette in the month before the survey.
Outcome measures: Social exchange scale, consisting of 16 items assessing aspects of social provision and acquisition of cigarettes.
Results: Almost 90% of youth in this study had obtained a cigarette from, and about 75% of them had provided cigarettes to, another teen in the prior month. Daily smokers provided to more teens and provided more often than those who smoked less than daily. Daily smokers also reported having more social sources, both teens and adults, than lighter smokers, and were more likely to have both bought from and sold cigarettes to other teens (p < 0.0001 for all comparisons between daily and less than daily smokers). In a multivariate analysis, social exchange was associated with grade, whether siblings and friends smoke, level of smoking, age of smoking initiation, parental influences and community norms about teen smoking, and buying cigarettes.
Conclusions: Social provision and acquisition of cigarettes among teens are widespread, reciprocal behaviours. Parental and community expectations about smoking influence social exchange, possibly by providing opportunities or barriers for social smoking. Commercial and social availability are not mutually exclusive; rather social exchange extends the reach of commercial sources.
- youth
- social sources
- ASSIST, American Stop Smoking Intervention Study
- TFF, Tobacco Free Future
- TPOP, Tobacco Policy Options for Prevention
- YRBS, Youth Risk Behavior Survey
Statistics from Altmetric.com
- ASSIST, American Stop Smoking Intervention Study
- TFF, Tobacco Free Future
- TPOP, Tobacco Policy Options for Prevention
- YRBS, Youth Risk Behavior Survey
The prevalence of tobacco use among adolescents is still unacceptably high, despite recent declines in smoking among this age group, and represents a significant public health challenge.1,2 Since the 1980s when it became clear that school based, tobacco use prevention programmes alone were not sufficient to reduce tobacco use among youth, prevention efforts have incorporated elements to influence the social context of tobacco use, including the availability of tobacco.3,4 The Centers for Disease Control and Prevention includes measures to reduce social and commercial availability of tobacco to youth in its recommendations for a comprehensive tobacco control programme.5
The first studies of availability of cigarettes for teenagers reported that commercial sources (businesses and vending machines) were most important, especially for regular smokers.6–11 However, more recent studies show that teens increasingly rely on non-commercial sources, including friends and other underage youth and adults who (knowingly or not) provide cigarettes to underage youth or purchase cigarettes for them.12 A survey of over 6000 students in grades 8–10 (ages 13–16 years) in 14 Minnesota communities revealed that 74% of the ever-smokers obtained their most recent cigarette from a social source.13 The 1997 Youth Risk Behavior Survey (YRBS) showed that about 70% of current smokers (at least one cigarette in the previous month) had obtained all their cigarettes from non-commercial sources.14 The Minnesota Student Survey asked about sources of tobacco in 1998 and 2001. The results showed that commercial sources were important only for the 12th grade students (ages 17–18 years), while students in grade 6 (ages 11–12 years) and grade 9 (ages 14–15 years) rely on friends and other social sources.15,16 Research based on a California survey of adolescents (the California Tobacco Survey) provides more detail on acquisition patterns analysed by smoking history.17 More than 90% of experimenters (< 100 cigarettes in their lifetime) usually were given their cigarettes. However, among established smokers, the majority either bought their cigarettes themselves or through an intermediary. The Legacy Foundation’s 1999 National Youth Tobacco Survey revealed that businesses were the usual and immediate source of cigarettes for only 10% of students in middle school and 26% of students in high school who reported past-month smoking.18 Finally, Jones and colleagues19 analysed the acquisition patterns of respondents to the YRBS for the years 1995, 1997, and 1999. They found a significant linear decline in the proportion of past 30 day smokers who usually bought their cigarettes in a store, and an increase in those who usually gave someone else money to buy them over the five year period.
This increase in use of non-commercial sources of tobacco can be linked to greater restrictions on commercial availability of tobacco to youth. Focus groups of adolescent smokers showed that youth under restrictive policies develop a complex system of obtaining and exchanging cigarettes, involving friends and strangers who have greater commercial access.20,21 In a randomised community trial, teen smokers in the towns where commercial access ordinances were adopted and enforced were more likely to have obtained their most recent cigarette from a social source than smokers in the control towns, and were less likely to have attempted to buy cigarettes.22 In another evaluation of local efforts to promote merchant compliance with state laws restricting commercial access by youth, teen smokers were more likely to report asking someone else to buy cigarettes for them in intervention counties compared to control counties.23
Data from studies in Minnesota and California both reveal that commercial and social sources are linked. These studies found that adolescents who provided cigarettes to other youth were more likely to have purchased their last cigarette.17,24 It has also been observed that teen providers were more likely to have a parent who smokes than non-providers.24 These data suggest that youth who provide to other youth are likely to obtain their cigarettes from an adult, either commercially or socially.
Whereas commercial availability primarily refers to opportunities to obtain tobacco from businesses, social availability includes both provision and acquisition, and may be linked to other potent aspects of an adolescent’s world, including the role models, normative expectations, social support, and social opportunities and barriers in their environment3,25 that have been found to be predictive of adolescent problem behaviours.26 To capture the broad set of influences on social acquisition and provision patterns, we have defined social availability of tobacco for youth as consisting of the non-commercial sources that provide tobacco (parents, other adults, same age friends, older adolescents), the opportunities to use tobacco (home and other private locations and public places where it is possible/acceptable for youth to use tobacco), role models that define use as desirable or appropriate behaviour (parents, other adults, older adolescents, and peers who use tobacco around adolescents), and community standards that support tobacco use as acceptable or at least normative for adolescents as well as adults.27 Public and private places where youth and adults are permitted to smoke or where youth perceive that it is ok to smoke (homes, worksites, recreation areas, schools) also may provide increased opportunities for social exchange. Observation of youth and adult role models smoking in various locations also may expand the range of locations where it is perceived that smoking is acceptable, and where negative outcomes of smoking are negligible. In other words, social availability as we have defined it here includes all aspects of the adolescents’ social environment within their communities that allow or promote tobacco use: sources of tobacco, places to use it, and reasons to use it.
The purposes of this study are to describe in more detail the process of social acquisition and social provision of cigarettes for teenagers, and to test our model of social availability as described above. Specifically we address the questions: from whom do teens obtain tobacco, and to whom do they provide it? We also test the hypotheses that social exchange of cigarettes is linked to community norms about teen tobacco use, opportunities to use tobacco, and adult role models of tobacco use. Finally, we examine the relation between social and commercial sources of cigarettes for teens.
METHODS
Communities
Students in 29 Minnesota communities are included in this study. Fourteen communities are part of the Tobacco Policy Options for Prevention (TPOP) study described previously,13,22 and 15 communities are part of the Tobacco Free Future (TFF) study. The 29 cities in the two studies include rural, suburban, and outstate urban communities with a median population of 9800 and a population range from 3228 to 86 918. For both studies, city selection criteria included a requirement that city schools had at least 90 students in each of grades 8, 9, and 10. In addition, the TPOP study excluded cities that were within the primary ASSIST programme region of the state, and the TFF study required that cities have adopted or be in the process of adopting commercial youth access ordinances. Cities were ordered according to the proportion of students in the schools who lived within city limits, and the school system in each was contacted for permission to survey students. A combined total of 53% of the school districts contacted agreed to participate in the study. While not statistically representative of the state, the cities in these studies are located in all regions of Minnesota and include about 18% of Minnesota cities with population greater than 3000.
The communities varied with respect to their policies restricting youth access to tobacco, but were similar in other respects. None of the cities had considered clean indoor air policies before this survey, and all school districts had adopted tobacco-free policies for school buildings for everyone at all times, including staff, students, and visitors.
Survey procedures
The survey, using identical procedures and instruments for both studies, was part of the follow up data collection for the TPOP study, and constituted the baseline data collection for the TFF study. In the TPOP and smaller TFF communities, all students in each school in grades 8, 9, and 10 were invited to participate in the survey. In the larger communities with more than one school with those grades, a single representative school was selected for each grade. The student surveys were administered in spring 1998 by study staff in classroom settings. Expired air carbon monoxide was also measured to serve as a bogus pipeline. Parents were given the opportunity to refuse permission for their child to participate, and students were given the opportunity to decline to participate at the time the survey was administered. The institutional review board of the University of Minnesota approved this protocol. The response rate among parents and teens across all 29 communities was 90%. Over 92% the respondents self identified as white, 50% were female, and approximately a third were in each of the three grades. In total, 16 176 students were surveyed. The number of respondents from each of the 29 communities ranged from 172–864, with a median of 516.
Measures
Past-month smokers were identified via a question asking about smoking frequency. Smoking intensity was constructed for all past-month smokers using survey questions asking the number of cigarettes smoked in the past seven days, and in the past 24 hours in addition to smoking frequency. The student’s answers to each of these three questions were converted to cigarettes per week and averaged. Daily smokers were those whose smoking intensity was ⩾ 7, and less than daily smokers were past-month smokers with a smoking intensity of < 7.
Several variables reflecting respondents’ use of commercial sources of cigarettes were used in these analyses. Students were asked whether or not they usually buy their own cigarettes. Another variable was constructed by adding together the responses from the three questions about whether respondents ever bought cigarettes from a vending machine, ever bought from a store, or ever stole cigarettes from a store. This variable, ever commercial sources scale, ranges from 0–3 and has a mean (SD) of 0.67 (0.88).
In addition, for the purposes of data reduction, a series of factor analyses were performed to construct scales that reflect underlying theoretical concepts regarding aspects of social provision and social exchange. Table 1 shows the variables included in each scale.
Social exchange, parent influences, and teen norms scales
A scale measuring social provision of tobacco was constructed with a series of questions asking respondents if they had ever given cigarettes to someone under age 18, and if so, to whom (sibling, same age friend, younger friend, stranger), to how many different teens in the previous month, and how often they provided (from less than once per week to almost every day). Respondents were also asked if they had ever sold tobacco products to another teenager. The final scale consists of eight items that were summed, with a mean of 9.76 (5.27), a range of 0–20, and high internal consistency (Cronbach α = 0.84).
Another scale measuring social acquisition of tobacco was constructed from questions asking about whether respondents had obtained cigarettes from a variety of social sources. The final scale, after factor analysis, consists of nine items that were summed, assessing whether the respondent got their first and most recent cigarette from a friend; whether they have ever gotten cigarettes from a sibling, another teenager, a parent, another adult; whether they have ever stolen cigarettes from somewhere (not a business); the number of different teenagers they have gotten cigarettes from; and if they have ever bought cigarettes from another teen. The mean value of the scale is 8.1 (3.13) with a range of 0–15 and a high internal consistency (Cronbach α = 0.75).
The social acquisition and social provision scales were highly correlated (Pearson correlation coefficient 0.71) and so they were combined into a single scale, social exchange. Factor analysis revealed that all of the items from the two subscales loaded onto the combined scale except obtaining the first cigarette from a friend. The final social exchange scale consists of 16 items with mean 17.8 (7.9), a range of 0–35, and Cronbach α = 0.86.
A factor, which we called the parent influences toward smoking scale, including parent behaviour and parent rules regarding smoking emerged from exploratory factor analysis. This factor has a mean value of 26.4 (9.2), a range of 0–46 and Cronbach α = 0.90. Parent influences consists of 18 summed items including: parental smoking status; observed smoking in own and other homes by teens and adults including parents; observed smoking outside and in the car by parents; and parental rules about respondent, other teens, adult family members, and guests smoking in the house and in their car.
Another factor emerged from exploratory factor analysis consisting of responses to the question: Do most people think it is ok for teens to smoke cigarettes in these places? Respondents answered using a scale from 1 (most people think it’s ok) to 7 (most people think it’s NOT ok) regarding 12 locations: in their or another person’s home; in school or on or near school property; in a car with young people; at work; in fast food or other types of restaurants; in a shopping centre; in a recreation centre, video arcade, bowling alley or pool hall; and in outdoor gathering places. This factor, which we call the teen norms against smoking scale, has a mean value of 60.8 (20.9), a range of 1–84, and Cronbach α = 0.96.
Analysis
Bivariate tabular analysis was first conducted to examine the association between the items in the outcome subscales (social tobacco acquisition and social tobacco provision) and independent variables (level of smoking and grade) using Pearson’s χ2 for significance testing. We then analysed the relation between the social exchange scale and several predictor variables on student characteristics based on mixed model multiple regression. The analysis was performed using the SAS/STAT MIXED procedure, a mixed model regression program especially suited to analysis of data from designs involving nested random effects,28 whereas students surveyed from the same community exhibited similarity in their tobacco exchange behaviour.
PROC MIXED procedure takes into consideration the intraclass correlation in the analysis and adjusts the variance estimates properly.
RESULTS
Just over 25% of the students in the entire sample had smoked in the month before the survey, including 14% who reported smoking at least one cigarette per day. Of the 4124 past-month smokers included in these analyses, 25% were in grade 8, 34% in grade 9, and 42% in grade 10. They were evenly divided among males and females.
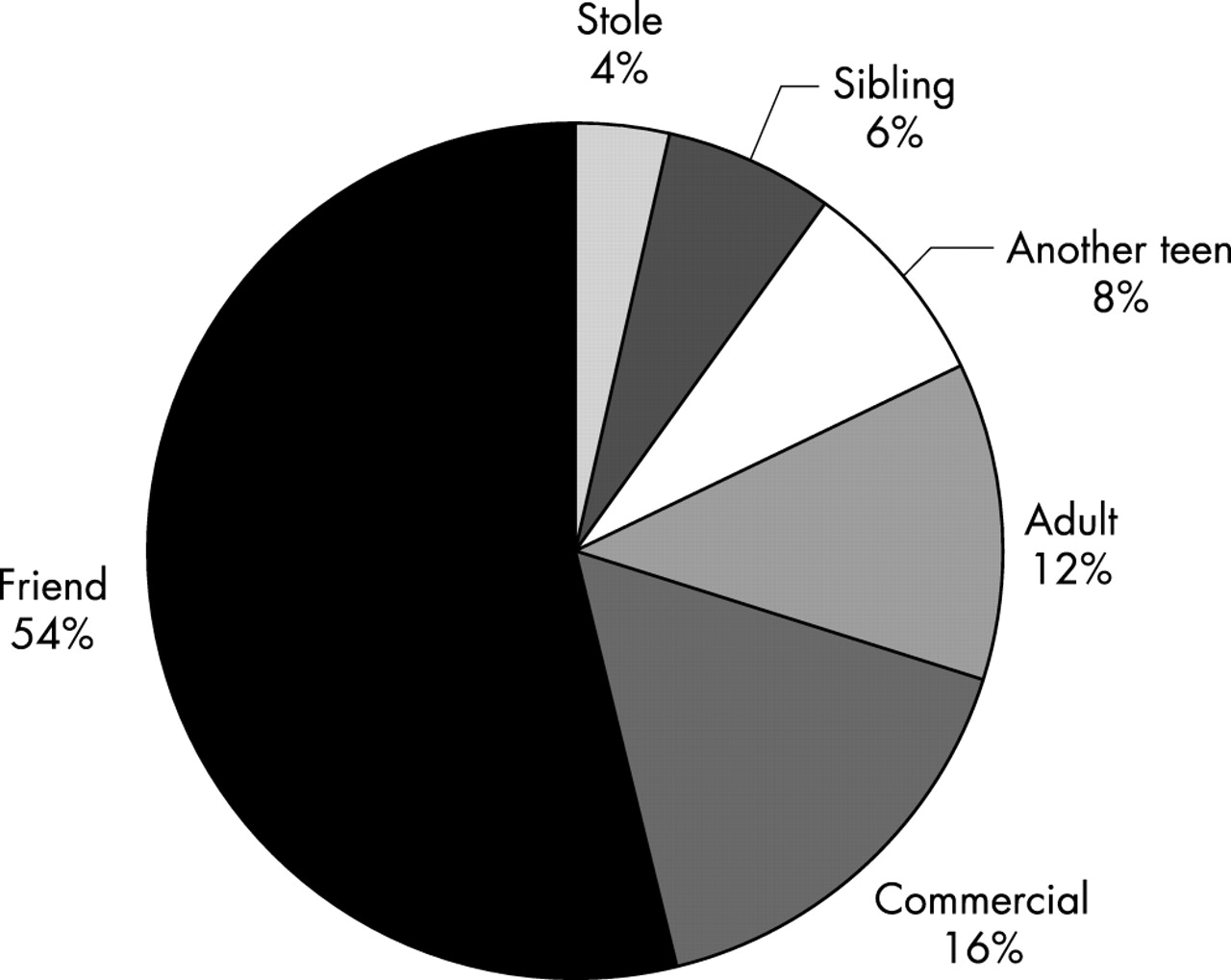
The majority of these past-month smokers had obtained their last cigarette from a social source. Figure 1 shows that 69% of them had obtained their last cigarette from another young person (sibling, friend or another teen) and 13% from a parent or other adult. Only 14% of them had obtained their last cigarette from a business (vending machine or over the counter).
{kind=link}
Source of most recent cigarette: past month smokers, grades 8–10 (n = 3991).
Table 2 provides more detail about cigarette sources. Eighty two per cent said that they had ever gotten cigarettes from another teen (not a sibling), while 25% had ever gotten cigarettes from a parent and 54% from another adult. Tenth graders were most likely to have gotten cigarettes from a parent, other teen, or other adult compared to younger respondents. Most reported getting cigarettes from at least two different teens in past month, with more than 28% having gotten cigarettes from at least six other youth. More than two thirds of past-month smokers had bought cigarettes informally from another teen. Between a quarter and a third of the past-month smokers reported having ever stolen cigarettes from someone (not a business), a behaviour more common among young compared to older respondents. Daily smokers reported using all sources and methods to get cigarettes more frequently than less intense or lighter smokers. There were no differences in social acquisition by sex.
Acquisition of tobacco from social sources, by grade and level of smoking
The respondents to this survey also provided cigarettes to other youth at high rates. Over 75% reported that they had given tobacco to another underage teen at least once (table 3), most often same age friends or acquaintances (64%). They were much less likely to have given tobacco to siblings (18%), younger acquaintances (27%) or strangers (14%). Daily smokers were much more likely to provide cigarettes to all categories of teens than were lighter smokers, and there were smaller but still significant differences by grade. About a third of respondents reported giving tobacco to two to five different teens and almost that many gave tobacco to more than five teens in the previous month. Many of them (50%) reported selling tobacco to other teens informally. Those who reported smoking daily were more likely to provide tobacco to a variety of teens and to provide more frequently compared to lighter smokers. Most past-month smokers provided tobacco to others less than once per week. Again, there were no differences in social provision by sex.
Provision of tobacco to other teens, by grade and level of smoking
Finally, we examined predictors of social exchange in a multivariate analysis. Grade, the parent influences scale, number of cigarettes smoked per week, age of initiation, whether their best friend smokes, whether a sibling smokes, what proportion of their friends smoke, the teen norm scale, whether they had ever obtained cigarettes commercially, whether they usually bought their own cigarettes, and whether they bought their last cigarette were all entered into a multiple regression analysis. All of those variables except sex were significantly associated with social exchange. Table 4 shows the final multiple regression model. Ninth graders, those who have a sibling who smokes, those whose best friend smokes, and those who usually bought their own cigarettes were more likely to participate in social exchange compared to other past month smokers. Stronger parent influences toward smoking, heavier smoking, earlier age of initiation, greater use of commercial sources, and less perceived community disapproval of teen smoking (teen norms against smoking) were associated with greater participation in social exchange. There was also a small but significant interaction between community disapproval of teen smoking and intensity of smoking.
Factors associated with social exchange among past-month smokers, grades 8–10*
DISCUSSION
This paper provides more detail about the phenomenon of social availability via social exchange—that is, acquiring cigarettes from, and providing cigarettes to, members of the social networks of teenagers who smoke. The data reported here indicate that teenagers use their social networks far more frequently than commercial outlets to obtain cigarettes. Most of their sources are other teenagers rather than adults, and parents are least likely to be a source of cigarettes.
Social provision and social acquisition are both widespread, prevalent behaviours among teens who smoke. Teens both give cigarettes to and get them from a large number of individuals. The fact that social acquisition and social provision are highly correlated indicates that these are largely reciprocal exchanges—that is, the same individuals who are providers also obtain cigarettes from social sources, and most teens who smoke have been both provider and recipient. Consistent with previously reported qualitative data,20 teens who smoke provide cigarettes less freely to siblings and younger teens than to others.
These data show that an informal (black) market for cigarettes clearly exists among teens, consistent with earlier qualitative information.12 More than two thirds of daily smokers have sold tobacco products to another teen, and most past-month smokers have bought them from another teen at least once.
These results confirm our initial hypotheses that social norms about teen smoking and opportunities to smoke are associated with social exchange. Perceived adult disapproval of teen smoking in various public places is negatively associated with social exchange, while parent influences toward smoking (lack of parental rules about smoking and parent smoking behaviour in various private locations) are positively associated with social exchange. These parent influences are not simply enabling teen smoking, since they predict social exchange independent of level of smoking, but also provide a social environment that allows exchange of cigarettes. Thus social exchange is not simply a situation where teens have access to another teen who provides or needs cigarettes. Rather, community and family attitudes and social environments, including an environment where commercial access is possible, contribute to the likelihood of social exchange occurring.
One of the most interesting results is the link between commercial access and social access to cigarettes for teens. Use of commercial sources is the strongest predictor of participation in social exchange. Thus social sources do not merely substitute for commercial sources, but extend their reach. As reported earlier, youth who reported buying their most recent cigarette were the most likely to report giving cigarettes to other teens.24
These findings call into question the assertion that efforts to reduce youth access to commercial sources should be abandoned in part because teens who smoke switch to social sources, and it is not feasible to reduce access from social sources.29,30 Our results show that social sources are dependent upon commercial access, and so reducing commercial access will reduce social sources. Furthermore, reducing commercial access forces youth who smoke to develop multiple strategies to obtain cigarettes, and possibly to smoke less or not at all. Finally, our results suggest several quite feasible strategies to reduce social exchange of cigarettes, and have a number of intervention implications:
-
Focusing only on convincing adults not to give cigarettes to teens will not significantly reduce social access. Adults are asked occasionally to purchase cigarettes for youth,31 but teens are a much more important social source of cigarettes for other teens than are adults. We must find ways to reduce the likelihood of teen-to-teen exchange.
-
Efforts to reduce social exchange must be broad based enough to affect a large number of teens, and must take into account the complex social factors that support teen smoking, since most teens who smoke participate in reciprocal social exchange, and the phenomenon appears to be integral to smoking behaviour. A narrow focus on social exchange behaviour is not likely to be successful, except possibly where strong norms already exist against providing to younger teens.
-
Heavier smokers are much more likely to both provide cigarettes to and get cigarettes from other teens, regardless of age. Daily smokers have more need for cigarettes, and so must develop more avenues for acquisition compared to those who smoke less than daily. Focusing on reducing the advance from occasional to regular smoking, as well as on preventing initiation, may have the additional advantage of reducing social exchange.
-
Social exchange is influenced by parent behaviour and expectations. Parents who smoke, who allow smoking in their home and automobiles by adults and youth, and who do not apply consequences to their child for smoking promote social exchange. Parents who enforce restrictive rules about not only youth smoking but also adult smoking restrict opportunities for social exchange in private settings, and reinforce negative expectations about smoking. This reduction in social access to cigarettes may account for part of the effect of strong parent rules on adolescent smoking reported by others.32,33
-
Social exchange of cigarettes among youth is influenced by community norms about smoking. Teens who believe that their community disapproves of their smoking in various public locations are less likely to participate in social exchange. This is a powerful finding because other studies have shown that most teen smoking occurs in public spaces.34 Teens are less likely to smoke in locations where they perceive it to be unacceptable, and thus less likely to have the opportunity for exchange. Restrictions on where people, including teens, can smoke in public may reduce social exchange for teens.
-
Restrictions on commercial sources may make social exchange more difficult and less likely. At the time of this survey, all of the cities in the survey had either adopted restrictions on youth access or were considering them. Also, the state of Minnesota had adopted a law the year before the survey requiring local jurisdictions to adopt and enforce a restrictive youth access law. Even under these circumstances commercial access was still a factor in social exchange.
What this paper adds
This paper defines social exchange, provides new information about the reciprocal nature of social acquisition and social provision, and new information about the relation between social and retail sources of tobacco to youth.
LIMITATIONS
The generalisability of these results is limited in several ways. The communities in the sample are limited to Minnesota, and the communities are a select sample of Minnesota communities. Thus these results may not be representative of the experiences of teens in all of Minnesota or in other states. The sample is further limited to students in grades 8, 9, and 10. Thus the experiences of older teens who smoke are not included. As noted above, the context for these findings is one in which strong restrictions to limit youth access to commercial sources of tobacco had already been implemented; these findings would not necessarily apply to situations where commercial sources were unrestricted.