Article Text

Abstract
Background: Smoking has been causally associated with increased mortality from several diseases, and has increased considerably in many developing countries in the past few decades. Mortality attributable to smoking in the year 2000 was estimated for adult males and females, including estimates by age and for specific diseases in 14 epidemiological subregions of the world.
Methods: Lung cancer mortality was used as an indirect marker of the accumulated hazard of smoking. Never-smoker lung cancer mortality was estimated based on the household use of coal with poor ventilation. Estimates of mortality caused by smoking were made for lung cancer, upper aerodigestive cancer, all other cancers, chronic obstructive pulmonary disease (COPD), other respiratory diseases, cardiovascular diseases, and selected other medical causes. Estimates were limited to ages 30 years and above.
Results: In 2000, an estimated 4.83 million premature deaths in the world were attributable to smoking, 2.41 million in developing countries and 2.43 million in industrialised countries. There were 3.84 million male deaths and 1.00 million female deaths attributable to smoking. 2.69 million smoking attributable deaths were between the ages of 30–69 years, and 2.14 million were 70 years of age and above. The leading causes of death from smoking in industrialised regions were cardiovascular diseases (1.02 million deaths), lung cancer (0.52 million deaths), and COPD (0.31 million deaths), and in the developing world cardiovascular diseases (0.67 million deaths), COPD (0.65 million deaths), and lung cancer (0.33 million deaths). The share of male and female deaths and younger and older adult deaths, and of various diseases in total smoking attributable deaths exhibited large inter-regional heterogeneity, especially in the developing world.
Conclusions: Smoking was an important cause of global mortality in 2000, affecting a large number of diseases. Age, sex, and disease patterns of smoking-caused mortality varied greatly across regions, due to both historical and current smoking patterns, and the presence of other risk factors that affect background mortality from specific diseases.
- CDC, Centres for Disease Control and Prevention
- COPD, chronic obstructive pulmonary disease
- CPS-II, American Cancer Society Cancer Prevention Study phase II
- GBD, Global Burden of Disease
- SIR, smoking impact ratio
- WHO, World Health Organization: AFR, African Region
- AMR, Region of the Americas
- EMR, Eastern Mediterranean Region
- EUR, European Region
- SEAR, South-East Asia Region
- WPR, Western Pacific Region
- cause of death
- developing countries
- global health
- risk assessment
Statistics from Altmetric.com
- CDC, Centres for Disease Control and Prevention
- COPD, chronic obstructive pulmonary disease
- CPS-II, American Cancer Society Cancer Prevention Study phase II
- GBD, Global Burden of Disease
- SIR, smoking impact ratio
- WHO, World Health Organization: AFR, African Region
- AMR, Region of the Americas
- EMR, Eastern Mediterranean Region
- EUR, European Region
- SEAR, South-East Asia Region
- WPR, Western Pacific Region
Smoking has been causally associated with substantially increased risk of premature mortality from several medical causes.1–3 In previous work,4 we estimated premature mortality attributable to smoking globally. There are, however, likely to be important differences in mortality effects of smoking in different populations, by geographical region, age, or sex, for example. These differences would arise from both differences in the accumulated hazards of smoking5 and differences in background (that is, non-smoker), disease specific mortality caused by other risk factors. For example, indoor cooking with coal, which is common in many parts of China,6 has given rise to higher background levels of mortality from lung cancer and chronic obstructive pulmonary disease (COPD), magnified by smoking.7 In other regions, exposure to multiple cardiovascular disease risk factors may make this group of diseases the most important cause of smoking attributable mortality.
Global estimates of mortality caused by smoking are important to provide the basis for international tobacco control efforts such as the Framework Convention on Tobacco Control.8 Disaggregated estimates, by region, age, and sex, also contribute to global tobacco control efforts by providing a means to document the shifting patterns of smoking and its associated hazards. Further, such disaggregated estimates can provide the evidence base for choosing interventions based on their expected effectiveness in various population subgroups. For example, taxation, advertising bans, and physician advice may have different effectiveness in different age groups, sexes, and socioeconomic circumstances. When coupled with detailed estimates of the health effects of smoking, the most effective or cost effective interventions can be selected to target those population subgroups where the hazards are concentrated. In this paper, we extend the global assessment of smoking-caused mortality, and provide estimates of smoking-attributable, disease-specific mortality for 14 epidemiological subregions of the world, separately for females and males and for younger (30–69 years) and older (70+) adults. Similar analysis at smaller scales (for example, for individual countries or even urban and rural parts of the same country) can provide more specific information for tobacco control policies and programmes.
METHODS
The hazards of smoking depend on factors such as the age at which smoking began, number of cigarettes smoked per day, cigarette characteristics such as tar and nicotine content or filter type, and smoking behaviour such as degree of inhalation.9 Many of these factors vary over time and across generations because of changes in the socioeconomic determinants of smoking including income, and tobacco control efforts such as tobacco trade and advertising laws, and prices and taxes. Therefore, current smoking prevalence or tobacco consumption alone would be insufficient indicators of the accumulated risk from smoking, even if detailed data were available in all countries. To overcome this difficulty, following Peto et al,10 we used lung cancer mortality as an indirect indicator of the accumulated hazards of smoking.
Background adjusted smoking impact ratio (SIR) was defined as the population lung cancer mortality in excess of never-smokers, relative to excess lung cancer mortality for a known reference group of smokers, adjusted to account for differences in never-smoker lung cancer mortality rates across populations (equation 1).5 Conceptually, by using excess lung cancer mortality as the indicator of the accumulated hazards of smoking in both study and reference populations, SIR converts the smokers in the study population—who may have different smoking histories—into equivalents of smokers in the reference population where hazards for other diseases have been measured.10 A detailed description of the use of SIR as a measure of exposure to accumulated smoking hazards with emphasis on developing countries is provided elsewhere5 and summarised below as appropriate.

-
CLC: age sex specific lung cancer mortality rate for 2000 in the study population (for example, country of analysis) from the World Health Organization’s Global Burden of Disease (GBD) database; see Mathers et al11 for methods
-
NLC: age-sex-specific lung cancer mortality rate of never-smokers in the same population
-
S*LC and N*LC: age-sex-specific lung cancer mortality rates for smokers and never-smokers in a reference population.
Peto et al10 used the same lung cancer mortality for never-smokers in the study and reference populations (numerator and denominator of equation 1), when applying the method to developed countries. Liu et al7 found that non-smokers in different geographical regions of China had lung cancer mortality rates that varied by a factor of 10 (see fig 4 in Liu et al7 and fig 1 in Ezzati et al5). The different non-smoker lung cancer mortality rates in China are largely a result of patterns of household energy use in China over the past few decades. Coal, a common household fuel in China and traditionally burned in stoves and buildings with poor ventilation, has been associated with increased lung cancer risk.12,13 Never-smoker lung cancer mortality rates in equation 1 for different regions were estimated based on the household use of coal in poorly vented stoves5 by using weighted averages of Chinese and American Cancer Society Cancer Prevention Study phase II (CPS-II) non-smoker lung cancer mortality rates, with weights corresponding to the prevalence of coal use. The remaining risk factors for lung cancer mortality (ambient air pollution, occupational hazards, indoor air pollution from radon or biomass smoke, etc) affect all populations in varying degrees. The net impacts of these other risk factors were considered as sources of uncertainty in never-smoker lung cancer mortality.4

Adult (30+) mortality caused by smoking in Global Burden of Disease (GBD) epidemiological subregions in 2000 for males and females, by age. See table 1 for definition of subregions.
Following Peto et al,10 we used CPS-II as the reference population, because CPS-II is one of the few studies of smoking and cause specific mortality conducted when the full effects of the smoking epidemic were apparent, especially for men. Therefore, the vast majority of (male) CPS-II current smokers had been lifelong cigarette smokers. Further, the estimates of increased risk of mortality among smokers were available for both men and women and in smaller age groups than in other studies.
Before using the CPS-II relative risks, we reduced the excess risk attributed to smoking using constant correction factors to avoid overestimating mortality caused by confounding in CPS-II risk estimates (which were initially adjusted for age and sex only) as well as extrapolation to other populations, where exposure to other risk factors could modify the effects of smoking in a non-multiplicative way.10 The correction factor used by Peto et al10 was 50% of excess risk. In subsequent studies, the overall effect of confounding from factors such as diet and alcohol has been estimated as considerably less than half of the excess risk for cardiovascular diseases (including evidence of negative confounding for some causes)14–17. In response to criticism about lack of empirical evidence for confounding correction,18,19 CPS-II data have been re-analysed with adjustment for potential confounders.20,21 In one re-analysis, except for cerebrovascular disease among men (where the fraction attributable to smoking decreased from 16% to 10%), adjustment for confounding had no or little effect on smoking attributable mortality (the next largest decrease was for lung cancer among men from 91% to 89% and COPD among women from 70% to 68%), or even resulted in a slight increase in risk for some causes.20 In a more detailed analysis, Thun et al21 adjusted for age, race, education, marital status, occupation (“blue collar” worker), and total weekly consumption of citrus fruits and vegetables in estimating the increased risk of mortality from a range of neoplasms, cardiovascular diseases, and respiratory diseases as a result of smoking. The analysis also adjusted for current aspirin use, alcohol consumption, body mass index (BMI), physical activity at work or leisure, and weekly consumption of fatty foods for cardiovascular diseases, and for occupational exposure to asbestos for lung cancer and COPD. With the exception of stroke among men, whose relative risk declined from 2.9 (2.3–3.7) to 2.4 (1.8–3.0) for those between 35 and 64 years of age and from 1.8 (1.6–2.2) to 1.5 (1.2–1.8) for those > 64 years, excess risks increased, stayed unchanged, or decreased by small amounts. Overall, adjustment for confounding reduced the estimates of mortality attributable to smoking in the USA by approximately 1%.21
Based on this new evidence on the robustness of CPS-II relative risks to adjustment for confounding, we used a correction factor of 30% (approximately equal to the largest reduction in excess risk after adjustment in the re-analysis of CPS-II) to reduce the excess risk for all cause-specific risks. This choice continues to be conservative to account for residual confounding or potential overestimation from extrapolation across regions. For the category “other medical causes”, where the extent of confounding is unknown, we attributed only half of the excess mortality estimated by CPS-II, following Peto et al.10 The excess risk in China was reduced by 5% to account for residual confounding. The proportional mortality method used by Liu et al7 is not affected by confounding due to any risk factor that increases mortality in the study and reference categories proportionally.
The age groups used in the analysis were 0–4, 5–14, 15–29, 30–44, 45–59, 60–69, 70–79, and 80+. No deaths before the age of 30 were attributed to smoking. SIR values were calculated for each age group and sex and for individual countries, and then averaged (population weighted) in each of 14 epidemiological subregions of the GBD project (see table1 for the list of countries in each subregion). The age-sex specific mortality statistics for the 191 WHO member states were from the GBD database. Details of mortality and cause-of-death analysis methods are provided elsewhere.11
RESULTS*
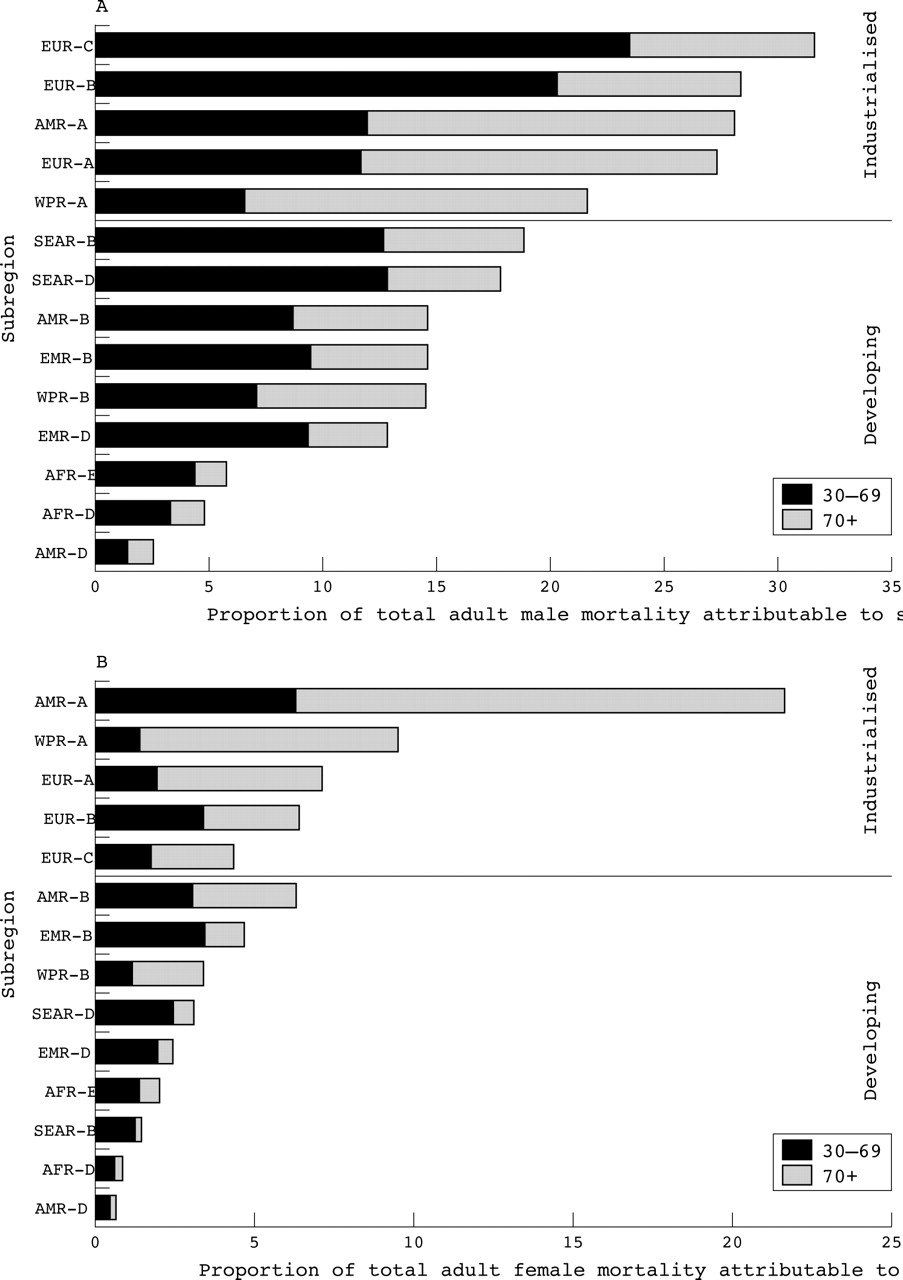
Globally, there were an estimated 4.83 million premature deaths attributable to smoking in 2000, 12% of total global adult (30+) mortality4; 3.84 million smoking-attributable deaths worldwide occurred among men and 1.0 million among women. The shares of adult male and female total mortality attributable to smoking were 18% and 5%, respectively. Figure 1 shows the breakdown of smoking attributable mortality for the 14 GBD epidemiological subregions by sex and broad age groups (30–69 and 70+). Figure 2 shows the fraction of total mortality attributable to smoking for men and women separately, also divided by the same age groups.

Fraction of total adult (30+) mortality caused by smoking in GBD epidemiological subregions in 2000, divided by broad age groups: (A) males; (B) females. See table 1 for definition of subregions.
As shown in fig 1, regions with the highest number of deaths attributable to smoking were the developing regions of South-East Asia (SEAR-D; dominated by India in terms of population) (0.68 million deaths) and the Western Pacific (WPR-B; dominated by China in terms of population) (0.65 million deaths), followed by a number of industrialised regions. This pattern, however, is partly because of the considerably larger population of these regions (table 1). When the proportion of total adult deaths that are attributable to smoking are considered (fig 2), the industrialised regions had the largest current effects, because of the longer history of smoking (see also fig 2 in Ezzati and Lopez5). At the same time, the increases in smoking over the last quarter of the 20th century have resulted in 10% or more of all adult deaths, and nearly 20% for adult men, now attributable to smoking in a number of developing regions.
Global burden of disease 2000 subregions
Overall, 75% of smoking-attributable deaths in industrialised countries and 84% in developing countries were among men. With the exception of North America (AMR-A), where women have smoked for several decades and female deaths accounted for 45% of total smoking-attributable deaths, current mortality attributable to smoking was concentrated more among men than women. In regions other than North America (AMR-A), the fraction of mortality caused by smoking that was among men ranged between 73% in the industrialised countries of the Western Pacific (WPR-A) to more than 90% in parts of South-East Asia (SEAR-B).
Relative to established market economies (AMR-A, EUR-A, and WPR-A), the industrialised regions of Eastern Europe (EUR-B and EUR-C) and developing countries had a higher proportion of smoking attributable mortality in the 30–69 age group, than at older ages (figs 1 and 2), resulting in a substantial number of life years lost to premature mortality. The share of adult smoking attributable deaths among the 30–69 age group ranged from a low 26% in the industrialised countries of the Western Pacific (WPR-A), 36% in North America (AMR-A), and 39% in Western Europe (EUR-A) to approximately 70% or more in sub-Saharan Africa (AFR-D and AFR-E), parts of the Eastern Mediterranean (EMR-D), parts of Eastern Europe (EUR-C), and South-East Asia (SEAR-B and SEAR-D). Overall, 62% of smoking attributable deaths in developing regions were between the ages of 30–69, compared to 49% in industrialised regions.
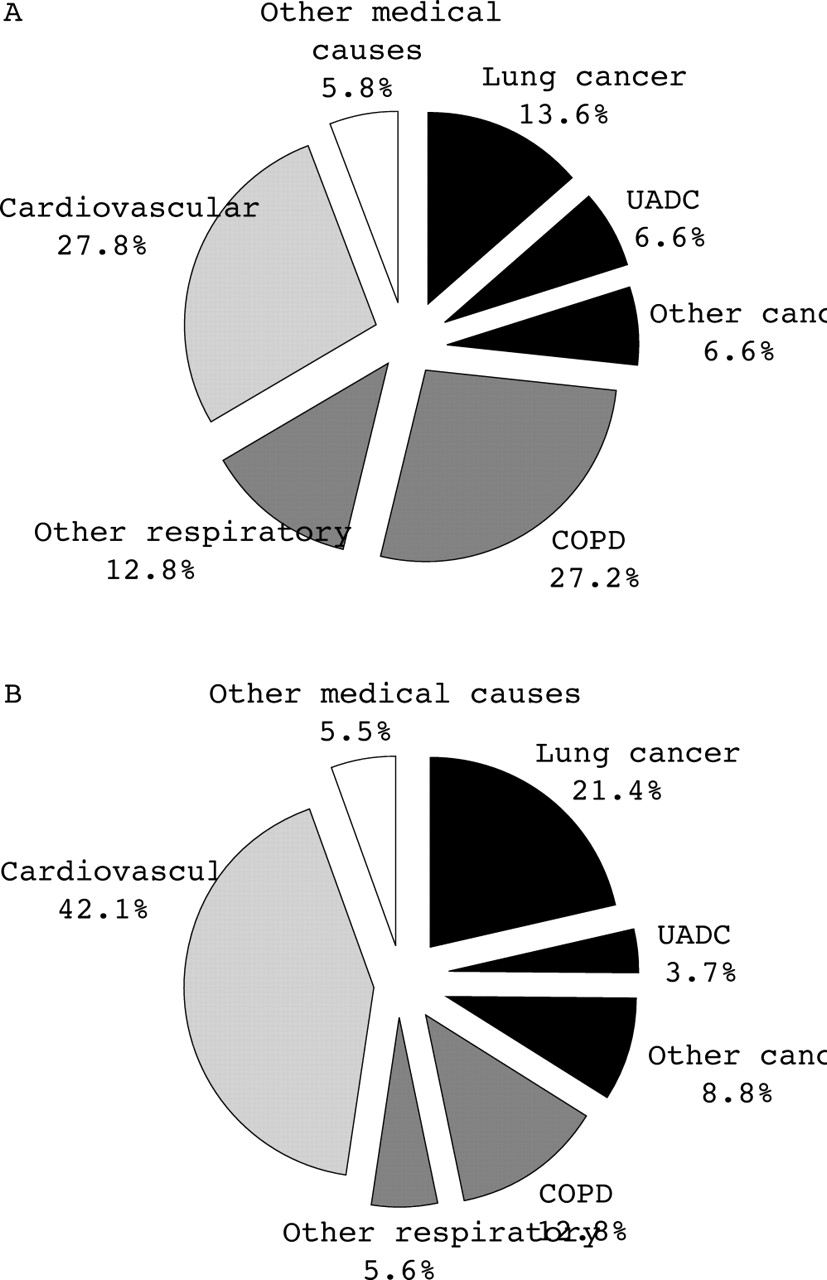
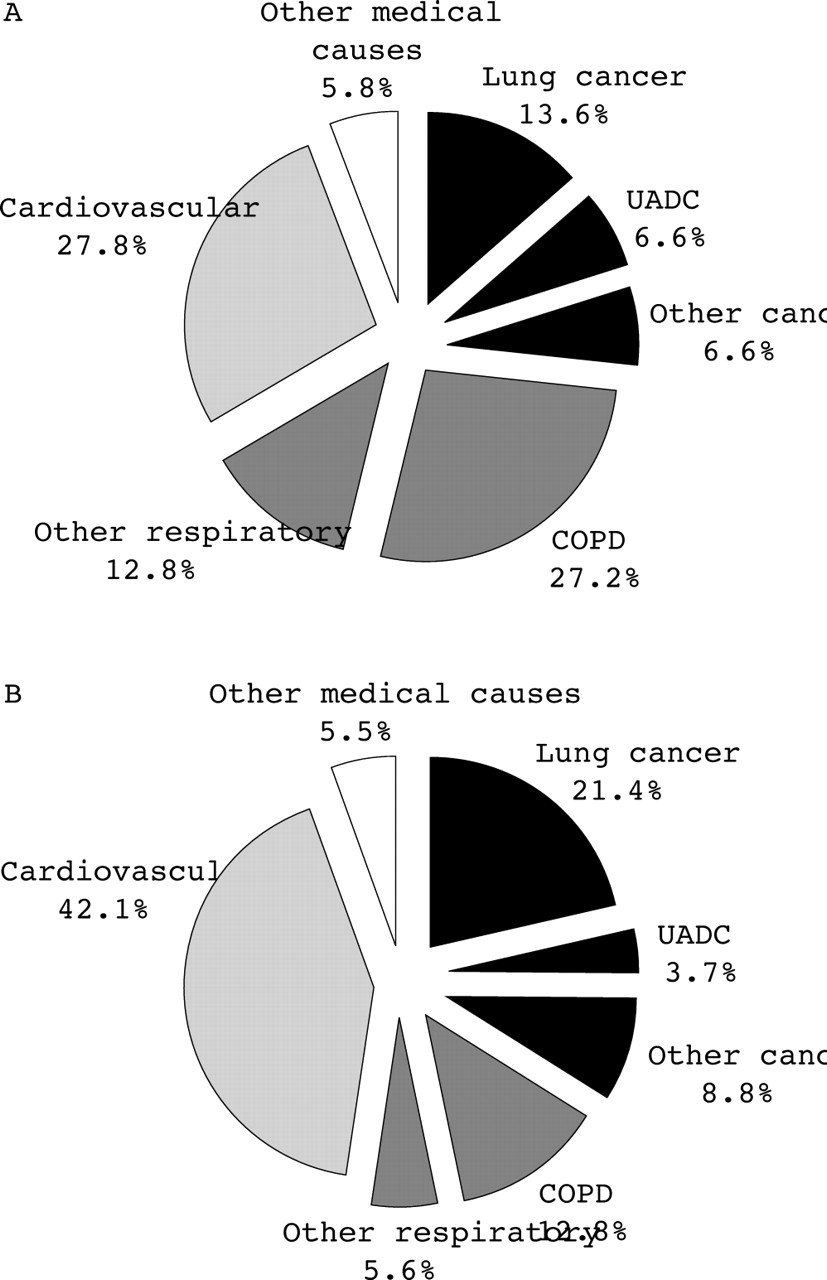
Figure 3 shows the contributions of different diseases, or groups of diseases, to smoking attributable mortality for the 14 GBD epidemiological subregions (table 1). The share of different diseases in total smoking attributable mortality is shown in fig 4 for developing and industrialised regions. Globally, the leading causes of death from smoking were cardiovascular diseases with 1.69 million deaths, COPD with 0.97 million deaths, and lung cancer with 0.85 million deaths. As we describe below, there were important differences among various industrialised and developing regions in the contribution of smoking to different diseases.

Mortality caused by smoking in 2000 in epidemiological subregions of the world by disease group. See table 2 in Ezzati and Lopez4 for details of disease groups. See table 1 for definition of regions. COPD, chronic obstructive pulmonary disease.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of mortality from smoking by cause. (A) Developing regions (total 2.41 million). (B) Industrialised regions (total 2.43 million). COPD, chronic obstructive pulmonary disease; UADC, upper aerodigestive cancer.
Mortality in industrialised regions (AMR-A, EUR-A, EUR-B, EUR-C, WPR-A)
The fraction of smoking attributable mortality in industrialised countries was highest in North America (AMR-A) where the 0.65 million annual smoking attributable deaths accounted for nearly 25% of total adult mortality. It was lowest in the industrialised countries of the Western Pacific (WPR-A) (16%). Among men, the fraction of smoking-attributable mortality was highest in EUR-C (dominated by Russia in terms of population) and North America (AMR-A), with 0.55 million and 0.37 million smoking-attributable male deaths, or 32% and 28% of all adult male deaths, respectively. Among women the highest fraction of smoking-attributable mortality was in North America (AMR-A), where 0.29 million adult deaths (21%) were attributable to smoking. Although women in some countries in Western Europe (EUR-A) have long smoking histories (for example, the UK), smoking is a more recent phenomenon in the southern parts of the continent, and therefore the share of female deaths in overall mortality currently attributable to smoking (7%) is still lower than in North America (AMR-A). Recent estimates suggest that this pattern is changing. For example, between 1990 and 2000, smoking attributable deaths among women in France and Italy rose from 2300 and 10 000 to 7800 and 14 000, respectively.23 The lowest fraction of male smoking-attributable mortality in industrialised countries was in the Western Pacific (WPR-A) (22%) and among women in Eastern Europe (EUR-B and EUR-C) (4%-6%).
For both males and females in all regions and age groups, lung cancer was the disease with the largest fraction caused by smoking, ranging from a low of 45% among females in EUR-C to a high of 91–94% among males in AMR-A, EUR-A, EUR-B, and EUR-C. Overall 92% of all lung cancer deaths among males (0.40 million lung cancer deaths) and 71% of all lung cancer deaths among females (0.12 million lung cancer deaths) in industrialised countries were attributable to smoking. Yet lung cancer accounted for only 22% of smoking-attributable deaths among men and 19% among women in industrialised regions. In fact, in the industrialised world, cardiovascular diseases were the leading cause of death attributable to smoking (see fig 3 and 4) and accounted for 42% and 44% of deaths attributable to smoking among men and women, respectively (0.75 million male deaths and 0.27 million female deaths from cardiovascular diseases caused by smoking). In Eastern Europe (EUR-B and EUR-C), where other cardiovascular disease risk factors such as elevated blood pressure and cholesterol are prevalent and important causes of disease burden,24 cardiovascular diseases accounted for an even higher proportion of smoking attributable mortality (53% in EUR-B and 56% in EUR-C) (fig 3).
When all cancers were considered together, the number of deaths caused by smoking approached that for cardiovascular diseases for men. Neoplasm deaths accounted for 37% and 26% of all smoking-caused deaths among men and women, respectively, in industrialised countries (0.66 million male deaths and 0.16 million female deaths from all cancers caused by smoking, accounting for 43% and 13% of all cancers among men and women, respectively).
Mortality in developing countries (AFR-D, AFR-E, AMR-B, AMR-D, EMR-B, EMR-D, SEAR-B, SEAR-D, WPR-B)
In general, there was larger variation in the mortality caused by smoking among different regions of the developing world than industrialised regions, because of the variability in history and patterns of smoking, as well as background mortality from different diseases. The fraction of total adult mortality caused by smoking ranged from a low of 2–4% in sub-Saharan Africa (AFR-D, AFR-E) and parts of Latin America (AMR-D) to a high of 9–11% in other parts of Latin America (AMR-B), parts of the Eastern Mediterranean (EMR-B), South-East Asia (SEAR-B and SEAR-D), and parts of the Western Pacific (WPR-B). For males the lowest fraction of total mortality caused by smoking were seen in parts of Latin America (AMR-D) (3%), sub-Saharan Africa (AFR-D (5%), and AFR-E (6%)), reflecting the considerably shorter history, prevalence, and intensity of smoking (see Krishnan et al25 for a discussion of changing patterns). The highest fractions of adult male mortality caused by smoking were in South-East Asia (SEAR-B (19%) and SEAR-D (18%)), parts of Eastern Mediterranean (EMR-B) (15%), parts of Latin America (AMR-B) (15%), and parts of the Western Pacific (WPR-B) (15%). For females, the fraction of total mortality caused by smoking in 2000 was equal to, or below, 2% in AFR-D, AFR-E, AMR-D, EMR-D, and SEAR-B. The highest fractions of female mortality were in parts of Latin America (AMR-B) (6%) and parts of Eastern Mediterranean (EMR-B) (5%), reflecting more recent increases in female smoking in these regions, with modernisation and economic development.
In developing countries also, lung cancer was the disease with the highest fraction caused by smoking—55% of all lung cancers or 0.33 million deaths were attributable to smoking (67% or 0.29 million deaths among men and 25% or 39 000 deaths among women). But lung cancer accounted for only 14% of all smoking attributable mortality (14% among men and 10% among women), versus 21% in industrialised nations. As in the industrialised countries, cardiovascular diseases were the largest cause of death from smoking, but followed very closely by COPD—0.67 million cardiovascular deaths (0.57 million among men and 0.10 million among women) were caused by smoking accounting for 28% of all smoking attributable deaths (28% among men and 25% among women); 0.65 million COPD deaths (0.50 million among men and 0.16 million among women) were caused smoking accounting for 27% of all smoking attributable deaths (25% among men and 41% among women).
The contribution of COPD was highest in parts of the Western Pacific which include China (WPR-B), where it accounted for 35% of all smoking caused deaths (30% among men and 55% among women). The high contributions from COPD are consistent with direct observations of Liu et al7 in China, where the high background rates of COPD mortality caused by air pollution from household use of coal and biomass fuels are magnified by smoking and result in substantial mortality from this disease. In WPR-B, cardiovascular diseases accounted for only 18% of deaths attributable to smoking, considerably lower than the global and developing region averages (figs 3 and 4). The relatively lower contribution of cardiovascular diseases to smoking caused mortality—in developing regions as a whole and particularly apparent in WPR-B—compared to the 42% in industrialised countries is likely due to relatively lower overall cardiovascular disease mortality in most developing regions and the higher contribution from COPD (see SEAR-D in fig 3 for an exception). Increased exposure to other cardiovascular disease risk factors in developing countries (for example, obesity and dietary risks), even with similar attributable fractions, would result in a rise in smoking-caused mortality.
As in the global total and industrialised countries, when all cancers were considered together, they approached cardiovascular diseases and COPD as the largest causes of death from smoking; 0.65 million neoplasm deaths (16% of all cancer deaths; 0.58 million or 26% of all adult male cancer deaths and 69 000 or 4% of all adult female cancer deaths) were caused by smoking accounting for 27% of all smoking attributable deaths (29% among men and 18% among women).
DISCUSSION
Indirect methods to estimate smoking-attributable mortality overcome the problem of absence of detailed data on smoking history. At the same time, the indirect method involves large uncertainty, especially in developing countries where both complete mortality records and detailed studies of smoking risks are less common. Uncertainty due to a number of inputs for this indirect method—including population lung cancer mortality, never-smoker lung cancer mortality, and hazard correction factor—have been included in previous analysis,4 yielding uncertainty ranges of 1.80–3.15 million for smoking-attributable mortality in developing regions and 2.13–2.78 million in industrialised regions.4 In addition to the above sources of uncertainty, using lung cancer—which has a longer lag time than cardiovascular and many other diseases attributable to smoking—as the marker for accumulated smoking hazard, can result in an overestimation of risk where there has been a sharp decline in smoking, and underestimation of risk where there has been large increases in smoking. The former is likely to apply in North America and those countries in Western Europe (for example, the UK) where smoking has declined.
While this effect is partially or fully offset by continued choice of a conservative hazard correction factor, it may account for some of the differences between our estimates and direct estimates for countries like the USA as reported by the Centers for Disease Control and Prevention (CDC).26 The differences between our estimates and those of the CDC are also partly because the latter are based on current smoking,26 which unlike the smoking impact ratio, does not account for changes in factors affecting accumulated population hazard, especially if there has been large changes in population smoking patterns relative to the epidemiological studies that quantify hazards. On the other hand, the hazards of smoking may be underestimated in most developing countries, where smoking has been on the rise over the past few decades. For example, comparison with recent direct estimates of mortality from smoking in India show that our estimates are slightly lower than those observed in direct epidemiological studies,27 although the differences vary by disease and age group due to factors such as cause-of-death classification.
Despite the uncertainty associated with these estimates, they illustrate that in 2000 smoking was an important cause of premature mortality among men in all regions of the world, and among women in industrialised countries. Mortality caused by smoking, including its share of total mortality and sex or age patterns, exhibited large variation among different regions of the developing world (men: from ⩽ 5% of total mortality in parts of Latin America and sub-Saharan Africa to ⩾ 15% in south-east Asia, parts of Latin America and Eastern Mediterranean, and Western Pacific; women: from ⩽ 1% of total mortality in parts of Latin America and sub-Saharan Africa to ⩾ 5% in other parts of Latin America). This inter-regional variation, larger than for industrialised regions, arises because the shape and maturity of the smoking epidemic is highly affected by the varying economic and sociocultural determinants of smoking in these settings. Despite this variability, current mortality attributable to smoking in the developing world is highly concentrated among men and among younger adults (30–69 years of age).
What this paper adds
Recent research shows that in the year 2000 smoking caused an estimated 4.8 million deaths in the world. These estimates also illustrated that currently the number of smoking caused deaths are identical in developing and industrialised countries. Globally, the leading causes of death from smoking were cardiovascular diseases, COPD, and lung cancer. Previous estimates have been disaggregated either based on geographical region or based on disease type, but not both.
This study provides estimates of mortality attributable to smoking in the year 2000 for adult males and females, including estimates by age and by specific diseases or disease clusters in 14 epidemiological subregions of the world. This disaggregation is crucial to focus and evaluate regional tobacco control policies.
There was large variability in the contributions of various diseases to smoking attributable deaths. This is because smoking magnifies the hazards of other risk factors for many diseases (for example, cardiovascular diseases and COPD), and results in larger disease-specific mortality where other risks for such diseases are prevalent. In particular the role of indoor smoke from solid fuels as a risk factor for COPD, has resulted in higher background prevalence, and meant that COPD and cardiovascular diseases were of identical importance in terms of contributions to smoking attributable deaths in developing regions. In industrialised regions, cardiovascular diseases were the single most dominant disease-affected by smoking, especially in Eastern Europe where cardiovascular diseases and their risk factors are important causes of death.
As the hazards of smoking accumulate among those who began smoking in developing countries over the past few decades, coupled with shifting demographic and disease patterns, the health consequences of smoking, already an important global health hazard, will continue to grow unless effective interventions and policies that curb and reduce smoking among males and prevent increases among females in these countries are implemented. Preventive strategies should also take advantage of the inter-regional heterogeneity identified in this research to tailor interventions to local conditions, differentially emphasising interventions designed for different age groups or to facilitate the balance between smoking prevention and cessation.
Acknowledgments
This work has been sponsored by the National Institute on Aging Grant 1-PO1-AG17625.
REFERENCES
Footnotes
-
↵* Three significant digits are reported to limit discrepancies between components and totals as a result of rounding. The precision of estimates is considerably lower due to large uncertainty in the estimates, quantified elsewhere.4
-
Contributions: Both authors contributed to adapting the Peto-Lopez method to developing countries, designed the analysis, and wrote the paper. Majid Ezzati conducted data analysis.