Article Text

Abstract
Objectives We sought to evaluate changes in countries' enacting advertising bans after the effect of ratifying the WHO Framework Convention on Tobacco Control (FCTC).
Methods We compared adoption of advertising bans on five areas (TV and radio, print media, billboards, point-of-sale, sponsorship) in countries that did versus did not ratify the FCTC, accounting for years since the ratification of the Convention.
Results On average, passage of complete advertising bans accelerated after FCTC ratification. The development was strongest among lower middle-income countries. Lack of state capacity was associated with lower likelihood of countries implementing complete advertising bans. Implementation of complete advertising bans slowed after 2007.
Conclusions Implementation of FCTC Article 13 was followed by increased progress towards complete advertising bans, but progress is incomplete, especially among low-income countries. Low-income countries need comprehensive support to implement FCTC as part of a broad effort to reinvigorate progress on global implementation of the FCTC. Enforcing complete bans requires constant monitoring and attacking of tobacco industry efforts to circumvent them.
- Advertising and Promotion
- Global health
- Low/Middle income country
- Public policy
Statistics from Altmetric.com
Introduction
The tobacco companies promote and perpetuate tobacco addiction through advertising, promotion and sponsorship1 (TAPS). Comprehensive TAPS bans reduce tobacco use, especially among young people, while partial advertising bans provide opportunities for tobacco companies to find new ways to market their products.2 The WHO Framework Convention on Tobacco Control3 (FCTC) that had 180 parties as of June 20164 commits parties to implement tobacco control measures, including Article 13 to ‘undertake a comprehensive ban of all tobacco advertising, promotion and sponsorship’.3 Article 13 guidelines emphasise that ‘a ban on tobacco advertising, promotion and sponsorship is effective only if it has a broad scope’.5 Article 13 requires prohibition of TAPS ‘that promote a tobacco product by any means that are false, misleading or deceptive or likely to create an erroneous impression about its characteristics, health effects, hazards or emissions’. In absence of complete bans, Article 13 requires ‘that health or other appropriate warnings or messages accompany all tobacco advertising and, as appropriate, promotion and sponsorship; and restrict the use of direct or indirect incentives that encourage the purchase of tobacco products by the public’. The treaty commits parties to comply with Article 13 within 5 years.
FCTC ratification was followed by an acceleration in passage of health warning labels6 ,7 and smoke-free environments.8 Poorer countries with less state capacity7 and countries that had previously entered into voluntary warning label agreements with tobacco companies were less likely to have enacted such strong labels6 and progress on smoke-free laws slowed over time.8
The tobacco industry has a long history of undermining tobacco control efforts including TAPS bans.1 ,9 It has promoted voluntary agreements over legislation and sought loopholes to continue promoting tobacco products.6 ,9 ,10 Compared with other FCTC demand reduction provisions, the parties have been slow to adopt complete TAPS bans. WHO's 2015 Report on the Global Tobacco Epidemic showed that only 29 countries had passed complete TAPS bans by 2014, while 49 had complete smoke-free environments, 42 had strong graphic health warning labels and 33 had implemented a 75% or above tax rate on cigarettes.1
FCTC Article 22 obliges parties to report to the Convention Secretariat on FCTC implementation.3 According to 2014 FCTC Progress Report 91, 70% of reporting countries had implemented comprehensive TAPS bans. The reports to FCTC Convention Secretariat are, however, not externally validated. Indeed, the 2014 Progress Report recognises that ‘Parties’ definitions of a comprehensive ban on advertising, promotion and sponsorship vary and do not always cover all of the specific measures called for by the guidelines for implementation of Article 13’.11 WHO collects independent data on national TAPS bans from 3 to 5 in-country experts from health ministries, tobacco control non-governmental organisations, health professionals, public health academics and the WHO Country Office that it makes available as a report1 and data set.12
We used the WHO data set to assess the adoption of TAPS bans following FCTC ratification, focusing on five areas: tobacco advertising in national TV and radio, national print media, billboards, point-of-sale (POS) and sponsorship.
Methods
Data
Restrictions on different TAPS forms
We used the data set for the WHO Report on the Global Tobacco Epidemic 201512 (years 2007, 2010, 2012 and 2014).
To establish a pre-FCTC baseline we used information collected by the tobacco industry's International Tobacco Documentation Centre's13 for its 1997 Smoking Issues Status Book (SISB) that listed advertising and promotion regulations in 179 countries or autonomous regions14 for direct (TV, radio, movies, press, billboards and point-of-sale) and indirect (free cigarettes, sponsorship, and whether brand or company names are permissible on non-tobacco products) advertising. To create categories corresponding to WHO data, we collapsed bans on TV and radio (96 countries had TV bans and 87 countries had radio bans in 1997); information on TAPS bans for press, billboards, point-of-sale and sponsorship were used as reported. (We excluded eight jurisdictions, mostly autonomous territories of European countries that were not WHO members (Azores, Canary Islands, Channel Islands, Gibraltar, Hong Kong, Isle of Man, Netherlands Antilles and Taiwan), that were listed in SISB. We scored missing data as no restrictions.
We studied countries' direct (national television and radio; local magazines and newspapers; billboards and outdoor advertising; point of sale) and indirect (free distribution of tobacco products; promotional discounts; non-tobacco products identified with tobacco brand names (brand stretching); brand names of non-tobacco products used for tobacco products (brand-sharing); appearance of tobacco brands (product placement) or products in television or films; and sponsorship, including corporate social responsibility programmes) advertising bans. We used WHO assessments of overall compliance with Article 13 (all provisions considered together) from 2007 to 2014 in WHO data set.11 We averaged scores provided by WHO experts, scoring ‘high’ 10 and ‘minimal’ 0.
For 1997 we constructed a compliance score using the SISB, assigning a value of 1 for a ban, 0.5 for restrictions and 0 for no restrictions for the six direct advertising (TV, radio, movies, press, billboards and point-of-sale) and three indirect advertising (practice of offering cigarettes free of charge to smokers, sponsorship and whether brand or company names are permissible on non-tobacco products) venues, then averaged the scores.
Other variables
We used World Bank 2016 gross national income (GNI) categories15 for country income: low income (per capita GNI $1045 or less in 2014), middle income ($1045 but <$12 736), high income ($12 736 or more). Lower middle-income and upper middle-income economies were separated at $4125.
We used Marshall and Cole's16 state fragility index to quantify state capacity (or, more precisely, incapacity). This index ranks all countries with populations above 500 000 in four performance dimensions: security, political, economic and social. We averaged the 2007, 2010 and 2013 scores. (Sudan scored 23 while the 15 most stable countries scored 0). Fragility is closely associated with a state's capacity to make and implement public policy and their resilience in maintaining system coherence, cohesion, and quality of life.
Additional potential independent variables included whether the country was in the Organization for Economic Cooperation and Development, whether it was in the European Community in 2003 (when European Community became party to FCTC), whether English was the official language, whether there was a common law system, the number of years since universal suffrage, the number of years since independence and whether the country's tobacco industry operated under voluntary TAPS restrictions instead of a legal ban in 1997. None of these variables were statistically significant, so they were dropped from final analysis.
In 2003 the European Union became a Party to the treaty, which was equivalent to all its members ratifying FCTC. We tested if the fact that the country was a member of European Community in 2003 had an effect on the results. It did not.
Statistical analysis
Logistic regression was used with the presence of a ban in 2014 as the outcome variable. We studied the effect of the FCTC by calculating the number of years since FCTC ratification as of 2014. Countries that ratified FCTC in 2014 (El Salvador, Ethiopia and Zimbabwe), had signed but not ratified the FCTC as of the end of 2014 (Argentina, Cuba, Haiti, Morocco, Mozambique, Switzerland and USA), or had not signed or become parties to the FCTC by January 2016 (Andorra, Dominican Republic, Eritrea, Indonesia, Liechtenstein, Malawi, Monaco, Somalia) had years since ratification set to 0. Countries that had a TAPS ban in 1997 were excluded from the analysis (80 countries with television and radio ban, 45 countries with print media ban, 46 countries with billboard ban, 23 countries with point-of-sale ban and 21 countries with sponsorship ban).
We used Stata V.13.1 for the analysis.
Results
Descriptive statistics
Restrictions on different forms of TAPS
As of 1997 two-thirds of high-income countries, one-third of upper middle-income countries, and one-quarter of lower middle-income and low-income countries had implemented TV and radio advertising bans (table 1). By 2014 78% of countries had bans, including 58% of low-income countries. TV and radio was the only category with statistically significant differences by country income level in the logistic regression.
Bans on forms of TAPS by income group in 1997 and 2014
In 1997, print advertising bans were less frequent than TV and radio adverting bans, with 19% to 31% of countries having bans (table 1). One-third of upper middle-income countries had bans on print advertising, more often than among high-income countries. This situation had changed by 2014, when 55% to 75% had a ban. Again, low-income countries lagged the other countries.
Billboard and print media bans increased following FCTC ratification more than for other venues. In 1997 bans on billboards were more unevenly distributed by income group than bans on print media (table 1). Only 10% of lower middle-income countries had bans on billboards in 1997 compared with 34% of high-income countries. By 2014 72% of lower middle-income countries had bans, the largest increase in compliance across venues and income groups. Low-income countries remained behind others with only 52% having a ban, compared to 72–75% for other countries.
In 1997 point-of-sale bans were rare even among high-income countries, with only 14% having bans. In 2014 compliance (table 1) only ranged from 29% (low-income countries) to 45% (upper middle-income countries).
In 1997, there were even fewer sponsorship than point-of-sale bans, with the compliance ranging from 3% (one low-income country, Somalia) to 15% (table 1), and less than half the countries implementing bans in 2014. Upper and lower middle-income countries implemented bans more often than high-income countries.
Although absolute compliance was highest in high-income countries, between 1997 and 2014 the lower middle-income countries demonstrated the most increase in TAPS bans, with an average compliance improvement of 47 percentage points over the five venues. The corresponding figure for upper middle-income countries was 41 and for high-income countries 23. Low-income countries made the slowest progress with an average improvement of 27 percentage points from 1997 to 2014. The compliance rate in the 2014 upper middle-income group shows the highest level of achievement with an average compliance of 64%, closely followed by high-income countries (63%) and lower middle-income countries (61%). In 2014, low-income countries (45%) were lagging behind more affluent countries
Overall compliance with TAPS bans
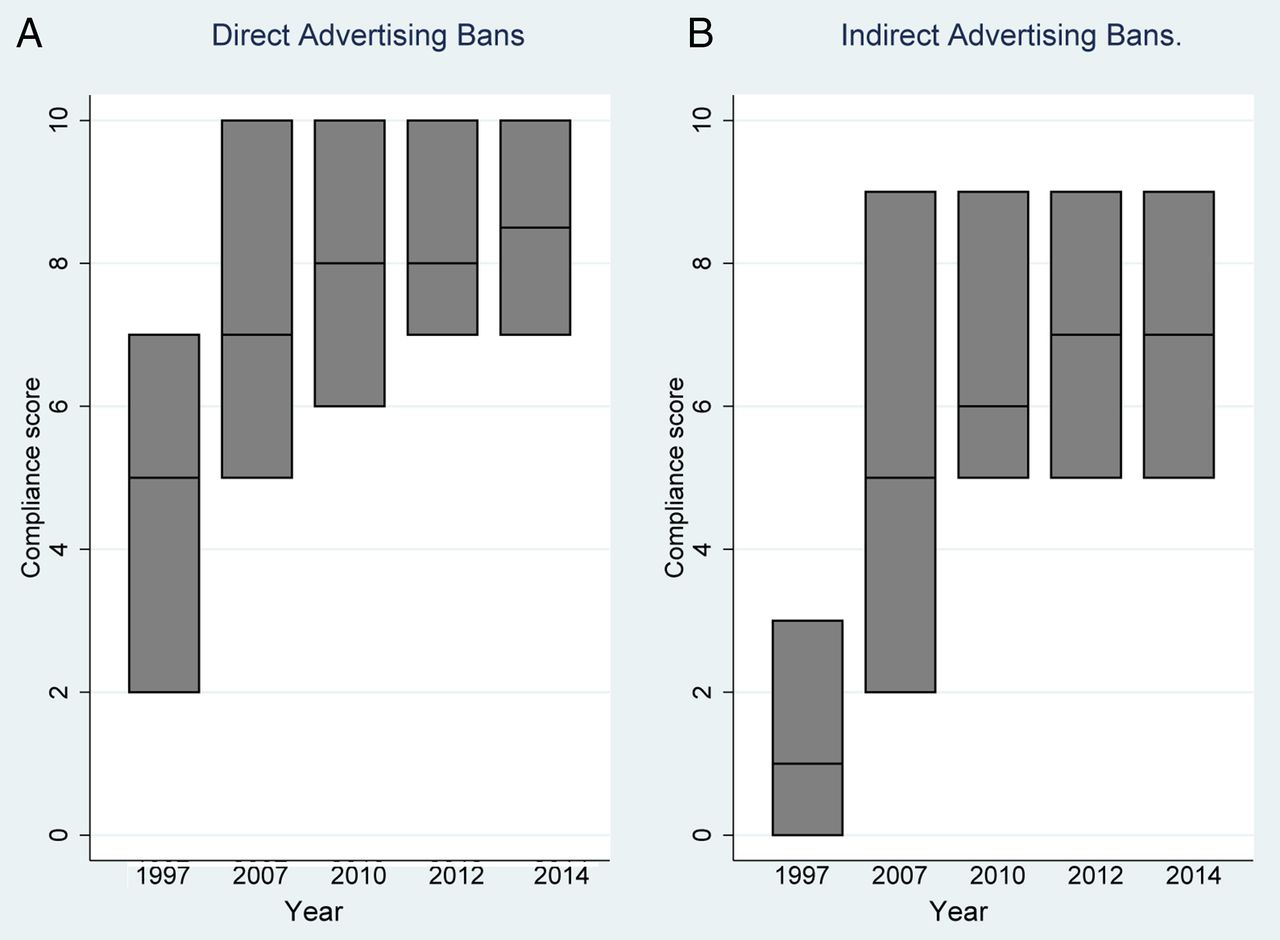
The rate of adoption of legislation for both direct and indirect advertising bans increased after the FCTC came into force in 2005 but had slowed by 2010 (figure 1). The overall compliance was higher for direct advertising than indirect advertising bans and increased rapidly from 1997 to 2007, then stabilised. The mix of income levels for countries in the sample did not vary significantly over time (p=0.219 for direct advertising score, p=0.177 for indirect advertising scores by χ2).

{kind=link}
Both direct and indirect advertising bans increased after the FCTC came into force in 2005 but progress had slowed by 2010. Boxes show median and 25th and 75thcentiles. FCTC, Framework Convention on Tobacco Control.
Logistic regression
FCTC ratification was followed by accelerated passing of television and radio advertising bans, print media advertising bans and billboard bans (table 2). Countries with less state capacity were less likely to pass complete bans. Income group was statistically significantly associated with the passing of TV and radio advertising bans.
Odds of passing advertising bans by 2014 (among countries that were non-compliant in 1997)
Discussion
Consistent with studies of health warnings6 ,7 and smoke-free laws,8 our analysis shows that FCTC ratification was followed by accelerated adoption of complete advertising bans on television and radio, national print media and billboards. By 2014 more than half the countries from all income groups had implemented complete bans on television, radio, national print media and billboard advertising. Before the FCTC high-income countries were ahead of low income and middle income countries (LMIC) in implementing TAPS bans. After the FCTC, lower middle and upper middle-income countries were more successful than high-income countries in implementing TAPS bans. Low-income countries lagged behind the others.
Compliance with the FCTC in 2014 was far from perfect. The lowest levels of compliance were observed for point-of-sale and sponsorship bans where the compliance rate by income group varied from 29% to 47%. As with smoke-free laws,8 progress towards full implementation has slowed as time passed since FCTC ratification.
While compliance with international treaties is less than perfect, ratification of a treaty is typically associated with a higher probability of implementing the policies the treaty specifies.17–19 Several mechanisms affect the link between FCTC ratification and implementation. The negotiations leading to the FCTC had an educational effect,20–22 increasing governments' awareness of the rationale for TAPS bans and contributing to implementing bans. Article 13 guidelines adopted in late 200823 were preceded by extensive negotiations between parties, which may also have raised awareness. In addition, the FCTC take effect for any party until 90 days after the 40th party ratified it, meaning that early ratifiers had almost two years before the FCTC came into legal force for them. Article 13.2 stipulates that parties implement a comprehensive advertising ban within five years after the FCTC entered into force. As a result, most of the progress occurred before parties were legally required to enact TAPS bans. The domestic political process necessary for ratification may have led political actors to understand the rationale for TAPS bans and increased adoption. Countries seek compliance with the treaties to varying degrees, so ratifying the FCTC may have led law-abiding countries to ban advertising. The FCTC reinforces the ‘ratchet effect’ of advertising bans, that is, following FCTC ratification, countries are less likely to reverse bans once they are adopted.
The Article 13 guidelines acknowledge that ‘the question of how constitutional principles are to be accommodated (in implementing comprehensive bans) is to be determined by each Party's constitutional system’.5 In 2014 six countries (Canada, Japan, Lao People's Democratic Republic, Marshall Islands, Poland and Uzbekistan) reported that constitutional limitations precluded them from implementing comprehensive advertising bans.11
We did not study the implementation of prohibition of display of tobacco products in retail sale facilities. By 2015, 35 countries had such bans.12
State capacity matters for passing FCTC-compliant TAPS bans. Producing better performance, however, may be difficult if a country's capacities to implement public policies in general are weak. The role of state capacity is also highlighted by the fact that more than half (69 of 130) countries reporting on FCTC implementation to the Convention Secretariat in 2014 referred to gaps between available resources—most often financial resources–as reasons for limited progress in FCTC implementation.11 Both results suggest that tobacco control measures are a part of broader societal development rather than a separate policy issue. An alternative explanation is that unstable countries may fail to implement Article 13 because, being in earlier stages of the tobacco epidemic, they view tobacco control as a low priority in a context of limited resources, not because they are incapable of implementing it.
Previous research identified LMICs as a priority for FCTC implementation.7 ,24 Five low-income countries have not ratified FCTC (Eritrea, Haiti, Malawi, Mozambique and Somalia). In 2006, New York Philanthropist Michael R Bloomberg launched a global initiative to reduce tobacco use in LMICs. Two years later the Bill and Melinda Gates Foundation joined the effort, focusing on Africa and Asia. Both organisations have supported efforts of some LMICs to comply with the FCTC.25 ,26 Costa Rica27 and Columbia (R Uang, E Crosbie, SA Glantz. Tobacco Control Law Implementation in a Middle Income Country: Tobacco Industry Opposition on Advertising, Ingredients, and Individual Cigarette Sales in Colombia. Global Public Health 2016;submitted) demonstrate that Bloomberg funding was instrumental to implementing FCTC. TAPS are most effective in LMICs.28 Low-income countries had the slowest progress in implementing TAPS bans and lowest compliance. TV and radio was the only category in which there were statistically significant differences in country income level in the logistic regression; the lack of statistical significant in other cases may be a statistical power issue.
Our results highlight the importance of focusing on low-income countries, where 622 million people lived in 2014. Of 31 low-income countries 26 were in Sub-Saharan Africa countries with young populations and low smoking rates, which make them attractive markets for tobacco companies.29 ,30
Enforcing complete TAPS bans requires constant monitoring of and response to tobacco industry efforts to circumvent bans.2 ,31 The industry has been particularly aggressive in fighting TAPS bans because advertising is essential for attracting new tobacco users to generate revenues and profits.1 Defining, implementing and enforcing TAPS bans is more difficult than reducing demand for tobacco through smoke-free laws and warning labels because tobacco promotion is an ever-changing target. The industry is constantly seeking new ways to promote its products, including cross-border advertising through international television and internet sites, mobile phones and sponsorship of international sporting and cultural events, including music events for young people.2 Other new forms of tobacco promotion, such as social media, may be hard to recognise, such as Imperial Tobacco's 2013 social media campaign (http://www.smoke-spots.co.uk/) to help smokers find ‘smoking-friendly places’.32
Other attempts to circumvent TAPS bans include promotional material including signage, poster boards and ashtrays. The companies use hard-to-track, ‘Corporate Social Responsibility’ (CSR) activities11 to improve their image with the public, press and regulators.30 ,33 By 2014 only eight countries explicitly banned tobacco companies from CSR activities, with six of them doing this as part of general bans on CSR.12
WHO experts' assessments founds that implementation of complete TAPS bans slowed after 2007, with shown weakening of complete TAPS bans over time. In 56 countries the assessment score for direct advertising in 2014 was lower than in previous years, while the corresponding figure for indirect advertising was 58. 30 countries reported having complete direct advertising bans (score 10) earlier but no longer in 2014. Since the WHO data are based on subjective assessments of the completeness of TAPS bans this finding does not necessarily mean that TAPS bans were revoked; it may rather reflect more rigorous assessments and the emergence of new forms of tobacco promotion not covered by previous laws. Across the five advertising areas in 195 countries in this study there were only three occasions in which a country revoked a ban. (Comoros's ban on print media tobacco advertising, Mali's ban on point-of-sale marketing and South Africa's ban on tobacco sponsorship were discontinued by 2010.) A more detailed country-by-country study would be required to determine if the tobacco industry is becoming more successful in blocking implementation of FCTC Article 13.
The FCTC does not currently have a clear mechanism to ensure that parties are notified when they are non-compliant. The FCTC Conference of the Parties (COP) established an expert group to review reporting arrangements that will make recommendation to the COP to be held in November 2016. It is imperative that a more formal validated reporting mechanism be implemented under the FCTC.
It is plausible that lack of POS advertising bans in low-income countries is due to fear of resource implications (the need to hire inspectors to check retail outlets regularly), but failure to ban sponsorship is unlikely to stem from resource concerns. The industry's use of sponsored organisations as proxies, ignorance that sponsorships are advertising and the smaller size of indirect that direct advertising when direct advertising is still allowed could contribute to this failure.
Limitations
We are unable to make causal claims concerning FCTC ratification and passing TAPS bans. Countries with pre-existing advertising bans may have been more likely to ratify the FCTC and some may have passed complete advertising bans in anticipation of FCTC ratification, which would lead us to underestimate the FCTC's effect. Almost all FCTC parties had ratified the treaty by 2006, which means that we are probably underestimating the effect of the FCTC on passage of complete advertising bans. Speed of ratification of the depends on the strength of the tobacco control advocacy community in a given country, as does adoption of a comprehensive TAPS ban.20 ,21
We were not able to verify SIBS data14 on advertising bans for 1997. We conducted a sensitivity analysis by recoding countries that SIBS reported as having ban in 1997 but which WHO did not report ban in 2007 as having no ban in 1997 (TV and radio 9 countries, print media 7 countries, billboards 12 countries, point-of-sale 11 countries and sponsorship 16 countries) with no substantial effect on the logistic regressions. Our analysis focused on five areas of tobacco advertising and did not cover all FCTC Article 13 provisions. The overall compliance score for 1997 is not directly comparable with compliance scores from later years because the 1997 score was based on assigning values for advertising bans covered in SIBS, while compliance scores for 2007, 2010, 2012 and 2014 were based on WHO experts' assessments.
Conclusions
FCTC ratification was followed by the accelerated passing of complete bans on different types of TAPS until about 2007, when progress slowed. Progress has been strongest among lower middle-income countries. Lack of state capacity was associated with lower odds implementing complete TAPS bans. Progress in Implementating FCTC Article 13 is incomplete, especially among low-income countries. Low-income countries need comprehensive support to implement TAPS bans as part of a broad effort to reinvigorate progress on global FCTC implementation.
What this paper adds
Compared with other demand reduction provisions of Framework Convention on Tobacco Control (FCTC), the Parties have been slow to adopt complete tobacco advertising, promotion and sponsorship bans.
Since adoption of FCTC lower middle-income countries have improved the coverage of TV and radio, print media, billboards, point-of-sale and sponsorship bans more than high-income countries or upper middle-income countries.
Implementation of complete advertising bans slowed after 2007.
In 2014 as many as 56 countries had weaker direct and 58 countries weaker indirect advertising bans than previously reported, suggesting that the tobacco industry is getting more successful in circumventing the bans.
References
Footnotes
Contributors HH developed the idea for this study and carried out the data collection. HH and SG carried out the data analysis and wrote and revised the manuscript.
Funding This work was supported in part by National Cancer Institute grant CA-087472. The funding agency played no role in the selection of the project, the conduct of the research, or the preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.