Article Text

Abstract
Background The US Food and Drug Administration (FDA) has regulatory authority to use inserts to communicate with consumers about harmful and potentially harmful constituents (HPHCs) in tobacco products; however, little is known about the most effective manner for presenting HPHC information.
Methods In a discrete choice experiment, participants evaluated eight choice sets, each of which showed two cigarette packages from four different brands and tar levels (high vs low), accompanied by an insert that included between-subject manipulations (ie, listing of HPHCs vs grouping by disease outcome and numeric values ascribed to HPHCs vs no numbers) and within-subject manipulations (ie, 1 of 4 warning topics; statement linking an HPHC with disease vs statement with no HPHC link). For each choice set, participants were asked: (1) which package is more harmful and (2) which motivates them to not smoke; each with a ’no difference' option. Alternative-specific logit models regressed choice on attribute levels.
Results 1212 participants were recruited from an online consumer panel (725 18–29-year-old smokers and susceptible non-smokers and 487 30–64-year-old smokers). Participants were more likely to endorse high-tar products as more harmful than low-tar products, with a greater effect when numeric HPHC information was present. Compared with a simple warning statement, the statement linking HPHCs with disease encouraged quit motivation.
Conclusions Numeric HPHC information on inserts appears to produce misunderstandings that some cigarettes are less harmful than others. Furthermore, brief narratives that link HPHCs to smoking-related disease may promote cessation versus communications that do not explicitly link HPHCs to disease.
- packaging and labelling
- public policy
- carcinogens
Statistics from Altmetric.com
Introduction
Product packaging and labelling can communicate to consumers the harmful and potentially harmful constituents (HPHCs) found in tobacco products and tobacco smoke.1–6 In many countries, tobacco packaging describes machine yields for some HPHCs (eg, carbon monoxide and nicotine) in specific brand varieties. However, presentation of quantitative levels of machine-assessed product yields for HPHCs can promote misperceptions that some cigarettes are less risky than others.7–13 In fact, cigarettes may be more harmful today than 50 years ago, despite dramatically lower machine-assessed HPHC yields.14 Indeed, there is no meaningful difference in the public health impact of different conventional combusted cigarettes (hereafter ‘cigarettes’) brands or their brand varieties.14 15 Because humans engage in compensatory smoking behaviours (eg, cover vent holes and inhale more deeply), machine yields often do not reflect human exposure to HPHCs.15 For these reasons, the WHO’s Framework Convention on Tobacco Control (FCTC) recommends that in addition to quantitative information about the levels of tobacco constituents and emissions, ‘qualitative statements […] about the emissions of the tobacco product’ be communicated to smokers, such as statement describing the link between exposure to constituents and the development of disease.16 Nevertheless, research is sorely needed to determine the most effective way to communicate about HPHCs.
Communicating public health messages through product packaging has a number of advantages, including the broad reach of information (ie, contact with tobacco consumers who buy packs), frequent exposures (eg, at purchase and during consumption) and low cost of dissemination (ie, paid for by the tobacco industry). For over 50 years, cigarette package exteriors have been used to communicate information on the consequences of smoking through health warning labels (HWLs).17 Over 100 countries have adopted prominent, pictorial HWLs,18 some of which integrate information on HPHCs. This strategy has increased smokers’ awareness of specific HPHCs,2–4 which appears to promote risk perceptions.
Aside from product packaging and HWLs, HPHC information could be included on ‘inserts’, which are small paper leaflets inside packages. In Canada, package inserts provide efficacy messages (ie, cessation tips and benefits of quitting), which complement prominent, pictorial HWLs that illustrate the health consequences of smoking.19 In the USA, the 2009 Family Smoking Prevention and Tobacco Control Act gave the US Food and Drug Administration (FDA) regulatory authority over the use of package inserts to communicate HPHC information to consumers if the agency determines that such information would benefit public health or otherwise increase consumer awareness of the health consequences of tobacco use.20
Inserts can communicate longer messages that are specific to brand varieties that HWLs could not accommodate. However, inserts must be designed to avoid consumer misinterpretations about varying levels of HPHC indicating different relative risks of cigarette varieties.
Information about HPHCs could also complement and reinforce information on HWLs. It is unclear whether specifically linking HPHCs to disease enhances risk perceptions relative to the mere mention of the presence of HPHCs in cigarettes or cigarette smoke. It is also unclear whether different ways of communicating the link between HPHCs and disease would influence perception of risks, including brief narratives of how the HPHC produces disease versus facts regarding where the HPHC is also encountered (eg, cyanide in rat poison). Research is needed to determine the effects of different ways that HPHCs in tobacco products can be represented in a format that is understandable and not misleading to a lay person.21
The US FDA’s list of HPHCs includes 93 constituents linked with five outcomes (ie, cancer, respiratory disease, cardiovascular disease, reproductive or developmental outcomes and addiction), for which industry must report to FDA on 20 HPHCs.22 Each of these health outcomes has an analogue in the mandated text for new cigarette HWLs that have yet to be implemented in the USA (eg, ‘Cigarettes cause cancer’). Prior consumer testing of HPHC information commissioned by the FDA examined consumer responses to listings of HPHCs.21 23 However, processing this information can impose a substantial cognitive burden for consumers that impedes their understanding of HPHCs and their related health risks. The current study included the following hypotheses:
numeric information regarding HPHC levels (vs no numeric information) will produce misperceptions that low-tar varieties of cigarette brands are less harmful than high-tar varieties;
grouping HPHC information by disease outcome (vs listing HPHCs alphabetically) will be more persuasive in motivating adults to not smoke;
compared with messages that do not link HPHCs to disease, messages that link HPHCs to disease outcomes will be more persuasive in motivating adults to not smoke;
the cancer diseases statement will lead to greater perception of harm and will be more persuasive in motivating adults to not smoke, compared with the other disease statements (ie, cardiovascular disease, lung disease and pregnancy-related adverse outcomes);
premium cigarette brands may be misperceived as less harmful than discount brands24 perhaps because they also perceive them as having higher quality and lighter taste.25
This study uses discrete choice experiments (DCEs) to determine the most effective manner for presenting HPHC information to promote consumer understanding of tobacco HPHCs and their effects. DCEs are commonly used in marketing research to test the influence of individual product attributes on consumer demand simultaneously and enable modelling of decision-making processes for product varieties that do not yet exist on the market.26
Methods
Participants
US adults (ages 18–64) were recruited using an online commercial panel from Lightspeed GMI. Panel participants were sent an email invitation that included a direct link to the survey and were reimbursed approximately $2 for completing it. Initial survey questions screened participants for inclusion criteria (aged ≥18 years) and quotas that would result in a minimum of 120 participants for each of the study’s 10 subgroups: six young adult (18–29 years) subgroups, stratified by smoking status (ie, susceptible non-smoker (ie, lack of a firm commitment to avoid smoking27); high-tar smoker; low-tar smoker) and educational attainment (ie, high school or less; greater than high school) and four older adult (ages 30–64 years) smoker subgroups, stratified by tar preference (ie, low vs high) and educational attainment (ie, high school or less; greater than high school).
Procedure and experimental design
We used DCEs,26 which presented cigarette brand varieties from the leading premium (ie, Marlboro and Camel), discount (ie, Basic) and in-between (ie, Pall Mall, positioned as premium quality at a discount price) brand families.28 Two different tar levels (ie, low vs high) within each brand family were presented along with pack inserts that communicated information about the HPHCs in that brand variety. Prior to the DCE, participants were shown a video clip explaining that the inserts they were about to compare emerged from the cigarette packages. The inserts included a warning statement about different disease outcomes (cancer, cardiovascular disease, lung disease and pregnancy outcomes), along with different kinds of information about HPHCs that were experimentally manipulated. All inserts included the same list of 16 HPHCs (see figure 1 and online supplementary file 1 for additional examples). These HPHCs were selected to represent the relative proportion of HPHCs that are associated with each of the disease outcomes assessed in our study. Where numeric HPHC levels were shown, the values used approximated known HPHC yields from machine testing,29 but they varied across brand varieties and were consistently lower for the low-tar varieties compared with high-tar varieties both within and across brand families.
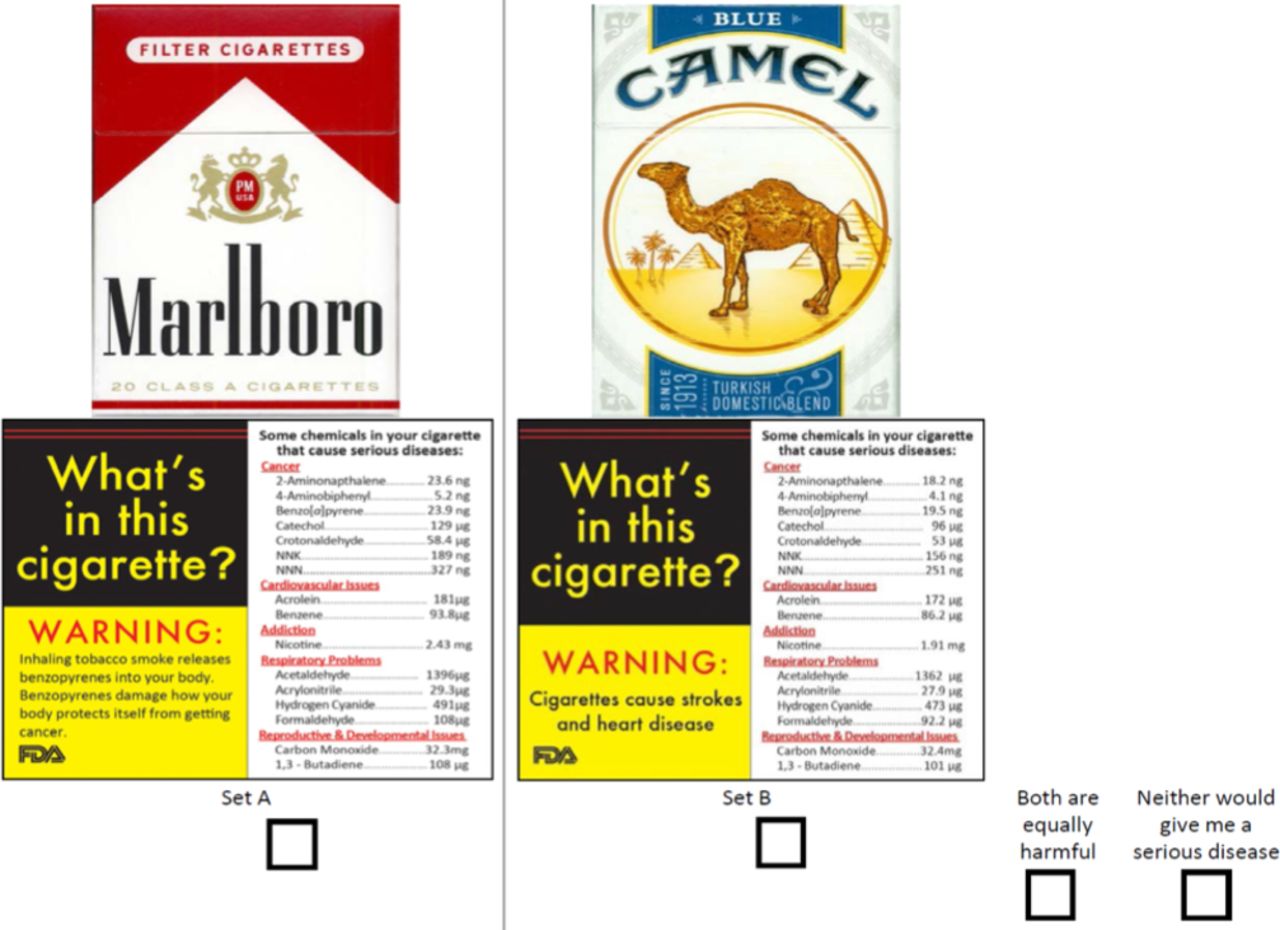
Sample choice set. Thinking about only yourself, which of these cigarettes would be more likely to give you a serious disease if you smoked them regularly?
The experiment involved a 4x2x4×2 (within subjects) combined with a 2×2 (between subjects) orthogonal design (see table 1) in which participants were asked to evaluate the difference between two sets of stimuli. Within-subject attributes included brand family (four brands) and tar level (high vs low), as well as health warning topic (four topics) and warning statement (presence vs absence of link to HPHC). The between-subject manipulations involved: (1) inclusion of numeric information about HPHCs versus no numeric information; (2) grouping of HPHCs by disease outcome with which the HPHC was primarily associated versus listing of HPHCs in alphabetical order. Online supplementary table 1 provides illustrative examples of the design differences for each attribute. The full factorial design generated 256 possible product combinations; however, to optimise the design and reduce response burden, each participant was randomised to evaluate one of 16 blocks of eight choice sets. Each choice set included two product combinations (left-side vs right-side choice) and two ‘no difference’ options. Our orthogonal and balanced design has desirable statistical properties and follows principles outlined by Louviere and Woodworth.30 The alternatives were pairwise independent of each other across choice sets. For each choice set, participants were asked the following questions: (1) ‘Thinking about only yourself, which of these cigarettes would be more likely to give you a serious disease if you smoked them regularly?’ and (2) ‘Which insert would most motivate you to not smoke cigarettes?’ For each question, participants could select: set A (left side), set B (right side), ‘both are equally harmful/motivating’ or ‘neither would give me a serious disease/motivate me to not smoke’. Respondents could view the choice sets for as long as they wished.
Discrete choice experiment design: product attributes and levels
Analyses
For each outcome (ie, [1] perception of relative harm and [2] motivation to quit), participants who chose a no-difference option across all eight choice sets were excluded from the primary analysis because they did not contribute meaningful information for analysing stimulus variables that influence choice. The demographic and smoking-related characteristics of excluded participants were compared with the analytic sample using Pearson’s χ2 tests and adjusted logistic regression in Stata V.14.
We analysed the DCE data using alternative-specific conditional logistic regression, with the choice as the dependent variable (ie, harm perception and motivation to quit), modelling the four distinct alternatives (ie, two product choices (left side and right side) and two no-difference options). This method has the advantage of allowing for both within-subject and between-subject variables to influence choice.31 It also allows testing for systematic bias in choosing the left-side versus right-side alternative. Independent variables included within-subject attributes: brand (four varieties, with Marlboro as the reference group due to its relatively greater popularity), tar level (high vs low), health warning topic (four outcomes, with cancer as the reference given relatively higher awareness of its association with smoking) and brief warning statement that explained how the HPHC was linked to the disease topic (vs simple warning statement that does not mention HPHCs). These models also examined the association of the between-subject attributes on choosing either one of the two product choices or ‘neither is harmful/motivating’ relative to ‘both are equally harmful/motivating’ as the reference category. The two between-subject attributes represented presence of numeric information (yes/no) and grouping of constituents by disease category (yes/no). The models also controlled for smoking status (ie, smoker vs susceptible non-smoker). To evaluate gender differences in response to pregnancy-related disease statement, we stratified analyses by gender.
To assess the influence of each attribute as a whole on consumer choice, a range of implied preferences (utilities) for each attribute was calculated, representing the difference between each attribute’s highest and lowest estimated part-worth utility. The relative importance of each attribute was then calculated as the range of estimated parameter values for each attribute, normalised by the sum of all the attribute ranges for a given outcome.
Results
Choosing ‘no difference’ options
A total of 1212 respondents completed the study, with 43% (n=519) indicating ‘no difference’ for all relative harm choices and 36% (n=438) doing so for all choices regarding motivation to not smoke (see table 2). Participants were more likely to choose the ‘no difference’ options for all eight choice sets for either outcome if they were: female (vs male); older adults (vs 18–24 years); black, Hispanic/Latino or of other race/ethnicity (vs white); and if they had higher education (vs lower education). Meanwhile, black participants were more likely than white participants to consistently choose ‘no difference’ options for the motivation to not smoke question. In terms of smoking status, smokers of all types were less likely than susceptible non-smokers to choose a ‘no difference’ option for all choice sets. Furthermore, choosing ‘no difference’ for all choices was more common among those not randomised to HPHC stimuli that included both numeric information and grouped the HPHCs by disease outcomes. In addition, 1150 participants (95% of the sample) accessed the questionnaire using either a desktop, laptop or large tablet, whereas 5% used a smartphone (small screen). We conducted a sensitivity analysis, which excluded participants who used a small screen, and found similar regression estimates with the adjusted sample (results not reported).
Sample characteristics (overall and stratified by ‘no difference’ choice) and logit models predicting ‘no difference’ for perceptions of harm and motivation to not smoke
Perceptions of relative product harm
Table 3 shows results from the DCE models for choices of insert comparisons with respect to harm perception. Overall, choices with the following attribute levels were perceived as having less harm: Pall Mall (ß=−0.223; SE=0.058; p<0.001) and Basic (ß=−0.318; SE=0.058; p<0.001) brands compared with Marlboro; low-tar brand varieties (ß=−0.118; SE=0.060; p=0.049) compared with high-tar varieties; and inserts with a pregnancy outcomes statement (ß=−0.172; SE=0.057; p=0.003) compared with the cancer statement. This finding was not gender specific. A statistically significant interaction between low-tar level and inclusion of numeric HPHC information on the insert (ß=−0.580; SE=0.084; p<0.001) indicated that numeric levels further promoted the perception of ‘low’ tar products as having relatively lower harm. Participants who were randomised to the numeric HPHC information condition were more likely to choose one of the two alternatives in the choice set rather than ‘no difference’: left-side choice (ß=0.289; SE=0.078; p<0.001) and right-side choice (ß=0.332; SE=0.076; p<0.001). Compared with smokers, susceptible non-smokers were significantly more likely to choose ‘both are equally harmful’ over the two product choices represented within each choice set: left-side choice (ß=−0.486; SE=0.085; p<0.001) and right-side choice (ß=−0.436; SE=0.082; p<0.001). Among the no difference options, participants were significantly more likely to choose ‘both are equally harmful’ over ‘neither are harmful’ (ß=−1.326; SE=0.376; p<0.001).
Estimated parameters of the alternative-specific conditional logit models predicting perceptions of product harm and motivation to not smoke
Motivation to not smoke
Table 3 also shows results from the DCE models for choices of which insert most motivated participants to not smoke. Results were similar to the models for relative harm, including an interaction between low-tar brand varieties and the provision of numeric HPHC levels ((ß=−0.276; SE=0.077; p<0.001) and pregnancy-related warning being less motivating than the warning about cancer (ß=−0.207; SE=0.055; p<0.001). This finding was not gender specific. The primary difference was that inserts with a warning message that explicitly linked the HPHC to the disease topic were perceived as more motivating (ß=0.182; SE=0.039; p<0.001). Participants who were randomised to the condition of grouping HPHC information by disease outcome were more likely to choose the right-side alternative over the no-difference alternative (ß=0.128; SE=0.063; p=0.030). Compared with smokers, susceptible non-smokers were significantly more likely to choose ‘both are equally motivating not to smoke’ over the left-side choice (ß=−0.340; SE=0.080; p<0.001), right-side choice (ß=−0.234; SE=0.077; p<0.001) and the ‘neither is motivating’ option (ß=−0.878; SE=0.195; p<0.001).
Relative importance of attributes
The relative importance of product attributes in predicting key outcomes is presented in figure 2, with estimates of the average relative weight that consumers placed on each attribute when forming their choices. With respect to perceptions of relative harm between product types, product tar level (42%) and brand family (34%) were the most important influences, with substantially less influence associated with the information on inserts (ie, disease outcome=19%; disease link to warning=4%). For choices involving insert messaging that motivated participants not to smoke, the disease topic on the warning was most influential (35%), with similar effects found for brand (23%), tar level (21%) and disease link (21%).

{kind=link}
{kind=link}
Relative importance of product attributes on key outcomes.
Discussion
To our knowledge, this is the first study to assess influences on consumer choice of different strategies to communicate HPHC information using discrete choice methods. Our findings are consistent with prior research that has found that communicating numeric information on HPHC levels across brand varieties promotes consumer misperceptions that some cigarette varieties are less harmful than others.32 33 Prior studies engaged smokers and ex-smokers in recalling the tar yield in their cigarettes and assessed whether their responses were ‘correct’7 10 or whether they had different interpretations of tar value.9 By contrast, this study involved a recognition task with presentation of products and accompanying inserts that included tar and 15 other HPHCs and probed smokers and non-smokers about their motivation to not smoke in addition to the assessment of perceived harm. The fact that we examined this in the context of a between-subject manipulation is a key strength of our study design over prior studies. Using between-subjects design allowed us to test a larger number of attributes without increasing response burden. ‘Correct’ responses involved indicating ‘no difference’ in harm between any product pair, indicated by almost half (43%) of participants. However, this response was more likely among those who were older, white and male, as well as those who were smokers, as opposed to susceptible non-smokers. Although participants with lower education were more likely to provide this ‘correct’ response, the overall pattern of results raises concerns that misperceptions of relative harm are more likely among vulnerable populations, including racial and ethnic minorities. Overall, these results provide support for WHO FCTC recommendations that communications about HPHCs do not include information about numeric levels.16
The findings indicate that different insert content and design attributes can motivate consumers not to smoke. Not surprisingly, different health warning topics were perceived as more or less motivating not to smoke, with messaging about pregnancy as the least motivating. Other research has found similar results, although this topic appears most effective among women of reproductive age.34 This underscores the importance of rotating health warning message topics, which may hold different appeal for different populations. More importantly, inserts that described how HPHCs led to disease outcomes were more effective at motivating participants not to smoke than inserts that did not describe the link between HPHCs and disease outcomes. However, we found smaller effects when HPHCs were grouped by the health outcome with which they were associated when compared with a simple listing in alphabetical order. Hence, the elaborated messaging strategy that states how HPHCs produce disease may be necessary to promote desired behaviours. Additional research is needed to examine whether this finding is reproducible in different samples and settings.
Randomising participants to the condition of grouping HPHC information by disease outcome did not yield significant differences in harm perception among product choices. With respect to motivation to not smoke, grouping HPHC information yielded significance with only the right-side alternative compared with the ‘no difference’ option. Although this finding may suggest a systematic bias towards choice of the right-side alternative, it is also plausible that this was a chance outcome of multiple comparisons given the large number of comparisons and the moderate p value. It is unclear from our findings whether grouping of constituents is a less effective communication strategy or whether redesigned inserts that place more emphasis on the grouping feature would yield different results. Future research that treats the grouping of constituents as a within-subjects design attribute would have more statistical power to explore this possibility.
The FDA’s authority to communicate about HPHCs for brands and sub-brands requires that the messaging does not produce misperceptions. Our results indicate that this would require eliminating quantitative information about HPHC levels. Since all cigarette brand varieties include the HPHCs about which FDA plans to communicate, in the absence of quantitative information, the same messaging would therefore apply across all cigarette brand varieties. Indeed, this would help underscore the primary public health message that all combustible cigarettes are equally dangerous. Future research should explore how consumers respond to HPHCs that apply across products, such as smokeless tobacco and electronic cigarettes, which may reduce harm from tobacco use precisely because they contain fewer HPHCs.
A key strength of this study was the use of DCEs, which is an established methodology that the tobacco industry itself has publicly asserted as the standard for simultaneous evaluation of the effects of diverse product attributes on consumer choice.35 It therefore provides potentially powerful premarket testing evidence for recommending public health communication strategies. Our protocol featured the presentation of cigarette packages paired with product inserts in order to test the effectiveness of various insert messages about HPHCs within the realistic context of popular premium and discount brand alternatives. Limitations of the design included the inability to assess all possible combinations of attributes. The inclusion of numeric HPHC information and the listing versus grouping of HPHCs by disease outcome were tested as between-subject manipulations, because we considered these to be specific policy configurations that would be best evaluated in this manner. However, given the complexity of the stimuli that participants evaluated, future studies may consider whether within subject manipulations of the grouping variable may be necessary to more fully explore its effects. Furthermore, more than one-third of participants were excluded from the DCE analyses for consistently choosing ‘no difference’ options. Although it is plausible that some participants purposefully indicated ‘no difference’ in harm and motivation to not smoke among the comparisons, the complexity of the tasks may be partially responsible; in which case, this would be reflective of a realistic scenario in which the consumer is uninterested in processing large volumes of information. Finally, since packages and inserts were shown to participants as two-dimensional images on a computer screen, interaction with the insert stimuli may have been different than in real life. However, efforts were made to convey insert functionality by including video clips that demonstrated inserts appearing from cigarette packages. Although DCEs estimate choice behaviour, they may be an imperfect predictor of behaviour, especially when there are barriers to the behaviour (eg, withdrawal symptoms and social drivers for smoking). Nevertheless, behavioural intention has repeatedly been shown to be a significant predictor of future behaviour.36
Conclusions
The findings of the current study can inform communication strategies for HPHC information, including the use of inserts in cigarette packaging, which allows for enhanced communication with smokers, including in the USA, where inserts may help address legal concerns about First Amendment rights that have delayed implementation of prominent pictorial HWLs printed on exterior cigarette packaging.37 A system to communicate HPHC information to the public could help underscore the potentially lower harm from using different kinds of tobacco products, such as smokeless products and electronic cigarettes, as many smokers are interested in reduced risk products but are confused about their relative harms. However, these communication efforts must avoid reinforcing misperceptions about some cigarette varieties being less harmful than others, which the tobacco industry has long exploited to reassure smokers who might otherwise quit using its products.38 Future research is needed on how to communicate about HPHCs in ways that promote correct perceptions of the relative risk of different nicotine products.
What this paper adds
Tobacco product inserts can be used to communicate with consumers about harmful and potentially harmful constituents (HPHCs) in tobacco products.
Statements linking HPHCs with disease outcomes can be used as a tool to enhance quit efficacy among consumers.
Presentation of numeric HPHC information may contribute to misperception of reduced harm for cigarette options with lower tar.
Acknowledgments
This research was supported by a grant from the U.S. National Cancer Institute (R01 CA167067). The funder had no role in the design, analysis, preparation, or decision to publish the manuscript.
References
Footnotes
Contributors JFT conceptualised and designed the project and obtained research funding. JFT, RGS and JJL contributed to the design of this study. RGS, JJL, KRG and FI were responsible for data analysis reported in this paper. All authors contributed to the interpretation of the findings. All authors contributed to successive drafts and approved the final manuscript.
Competing interests None declared.
Ethics approval University of South Carolina Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it was published Online First. The Acknowledgements statement has been added in.