Article Text

Abstract
Background Studies that assess waterpipe tobacco smoking behaviour and toxicant exposure generally use controlled laboratory environments with small samples that may not fully capture real-world variability in human behaviour and waterpipe products. This study aimed to conduct real-time sampling of waterpipe tobacco use in natural environments using an in situ device.
Methods We used the REALTIME sampling instrument: a validated, portable, self-powered device designed to sample automatically a fixed percentage of the aerosol flowing through the waterpipe mouthpiece during every puff. We recruited participants at café and home settings in Jordan and measured puffing behaviour in addition to inhalation exposure of total particulate matter (TPM), carbon monoxide (CO), nicotine, polycyclic aromatic hydrocarbons and volatile aldehydes. We correlated total inhaled volume with five selected toxicants and calculated the regression line of this relationship.
Results Averaged across 79 singleton sessions (52% male, mean age 27.0, 95% home sessions), sessions lasted 46.9 min and participants drew 290 puffs and inhaled 214 L per session. Mean quantities of inhaled toxicants per session were 1910 mg TPM, 259 mg CO, 5.0 mg nicotine, 117 ng benzo[a]pyrene and 198 ng formaldehyde. We found positive correlations between total inhaled volume and TPM (r=0.472; p<0.001), CO (r=0.751; p<0.001), nicotine (r=0.301, p=0.035) and formaldehyde (r=0.526; p<0.001), but a non-significant correlation for benzo[a]pyrene (r=0.289; p=0.056).
Conclusions In the natural environment, waterpipe tobacco users inhale large quantities of toxicants that induce tobacco-related disease, including cancer. Toxicant content per waterpipe session is at least equal, but for many toxicants several magnitudes of order higher, than that of a cigarette. Health warnings based on early controlled laboratory studies were well founded; if anything our findings suggest a greater exposure risk.
- carcinogens
- nicotine
- smoking topography
Statistics from Altmetric.com
Introduction
Waterpipe tobacco smoking is a generic term to describe the inhalation of charcoal and tobacco smoke that has passed through a water-containing instrument. Since the turn of the 21st century, the mass manufacture of Mo’assel tobacco, a product thought to contain 30% tobacco laced in molasses and glycerine,1 has contributed to substantial spread of waterpipe tobacco use in many settings globally.2 National estimates of current use (defined as at least once in the past 30 days) are high among young people in Middle Eastern settings (eg, Lebanon 37%, West Bank 33%, Syria 20% and Jordan 19%),3 Eastern European settings (eg, Latvia 23%, Czech Republic 22% and Estonia 22%)3 and of concern in other settings (eg, USA 11%, Germany 10% and Brazil 9%).4–6 Fuelling this popularity is the false belief that waterpipe tobacco contains fewer toxicants than cigarettes, or that toxicants are filtered out by the water through which the smoke passes.7
In recent years, a growing literature has begun to demonstrate that, contrary to common perception, waterpipe tobacco smoke contains and delivers considerable toxicant loads. Studies have found consistently high yields of ‘tar’ (800–2350 mg/session),8–12 carbon monoxide (CO) (60–370 mg/session),8–15 nicotine (1–8 mg/session)9–11 14 16 and cancer-causing agents such as benzo[a]pyrene (not detected to 300 ng/session) and formaldehyde (40–630 ng/session).17 Other harmful toxicants found within waterpipe tobacco smoke include tobacco-specific nitrosamines,18 primary aromatic amines,19 heavy metals16 20 and furanic,21 volatile organic22 and phenolic compounds.22 23 To meet scientific standards for replicability, smoking machine studies of waterpipe toxicant emissions require standardised test conditions and fixing of numerous variables. These variables include the amount and manner in which the tobacco is loaded into the device, the amount, type and timing at which charcoal is added, the geometry and materials of construction of the waterpipe, and the puffing regimen used to simulate smoking. To a large extent, the implications of the choices made by investigators are unknown, leaving uncertain the degree to which analytical laboratory measurements of toxicant emissions reflect real-world exposure, particularly given the highly idiosyncratic nature of waterpipe tobacco smoking. To take one example, waterpipe users commonly manipulate the several pieces of charcoal placed on the waterpipe head during a typical use session; for example, on multiple occasions they may pick up one or more pieces with tongs, blow on them to remove ash and return them to the waterpipe. They may also add new charcoal from a nearby fire box or remove charcoal to regulate the smoke density or flavour. Given that charcoal contributes more than 90% of the CO and benzo[a]pyrene in waterpipe smoke,13 the way that charcoal is applied in the analytical laboratory may influence resulting toxicant determinations. Any standard method adopted for laboratory testing purposes will involve a high degree of idealisation of real-time use patterns. As with the tobacco industry’s decades long effort to undercut tobacco control policy by creating scientific controversy,24 uncertainties deriving from the use of standardised testing methods have been exploited to sow doubt about the harmful nature of waterpipe smoke.25
An approach that may have more ecological validity involves sampling waterpipe smoke in real time, in the natural environment. We have reported the development and deployment of a device that can automatically sample a fraction of every puff drawn by a waterpipe user in natural settings.26 We piloted this approach in a sample of café smokers in Beirut, Lebanon, and on average measured 119 L of smoke, containing 602 mg of tar, 150 mg of CO and 4 mg of nicotine per use session, which on average lasted 61 min. While this study confirmed that real-world waterpipe use involves inhalation of large quantities of tar, nicotine and CO, specific toxicants such as acrolein, formaldehyde and benzo[a]pyrene that are associated with cancer and pulmonary disease were not examined. Concentrations of these toxicants in tobacco smoke are typically several orders of magnitude smaller than those of tar, nicotine and CO, and are therefore more challenging to measure. More pertinently, emissions of these toxicants may vary widely with small changes in waterpipe smoking conditions, and therefore the relevance of reported laboratory smoking machine yields of these smoke components to real-world exposure is particularly uncertain.
In the current study, we developed a second-generation automatic smoke sampling instrument, REALTIME and deployed it to determine inhalation exposure to 12 species of volatile aldehydes (VAs), 16 species of polycyclic aromatic hydrocarbons (PAHs), as well as nicotine, CO and total particulate matter (TPM). In addition to documenting real-world exposure to a wider range of toxicants, this study focused on home use, which has been reported as the main smoking location in a number of studies in Jordan and elsewhere.
Methods
REALTIME device
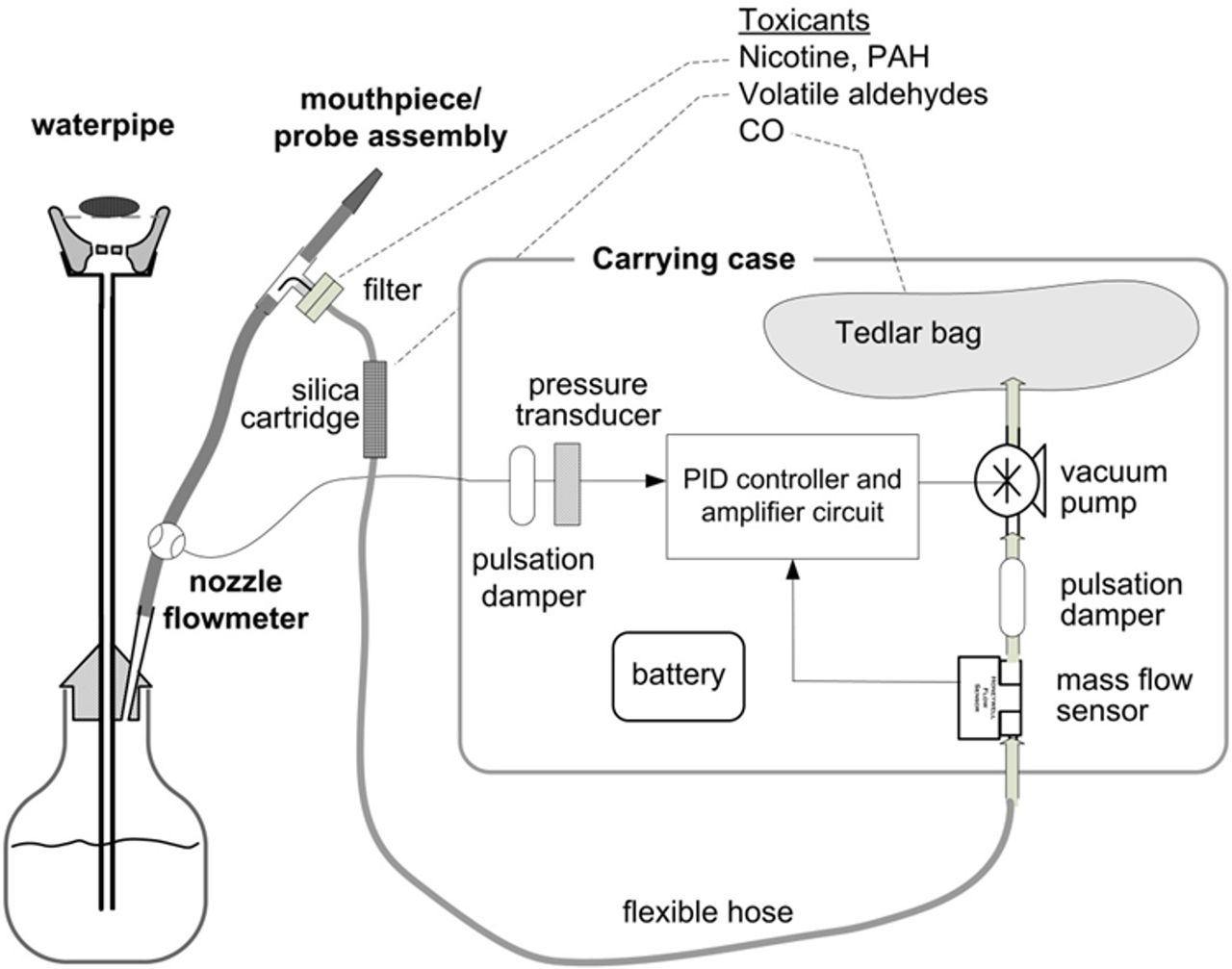
The REALTIME device used in this study had been described previously26 and is shown schematically in figure 1. In brief, REALTIME is a portable self-powered device designed to sample automatically a fixed percentage (5% in this study) of the aerosol flowing through the waterpipe mouthpiece during every puff. The sampled aerosol is drawn through a glass fibre filter trap (Pall Type A/E, 25 mm), followed by a 2,4-dinitrophenylhydrazine (DNPH)-coated silica cartridge (Sigma-Aldrich H10, 3 mL), and is then exhausted into an airtight Tedlar bag. This sampling arrangement allows for off-line quantification of PAH and nicotine (filter trap), VAs (silica cartridge) and CO (bag). The REALTIME device can only generate one sampled filter from each session. Each filter was analysed for either PAH or nicotine. We, therefore, randomly selected half the filters for each analyte.

Schematic of REALTIME smoke sampling apparatus. CO, carbon monoxide; PAH, polycyclic aromatic hydrocarbon, PID, proportional– integral –derivative.
REALTIME incorporates a calibrated flow sensor/nozzle embedded inline of the smoking stream in the waterpipe hose. During a smoking session, the flow through the waterpipe mouthpiece is monitored continuously (every 0.1 s), and is used as an input to a proportional–integral–derivative controller that activates a variable speed sampling pump whose instantaneous flow rate is also monitored, via a high-speed mass flow sensor. The electrical power to the pump is varied automatically by the circuit to ensure that the sample flow is always a fixed fraction of the mainstream smoke flow. This closed-loop control system operates at a rate of 200 samples per second.
The mainstream and sample stream flow rates are sampled continuously, digitised and recorded by an automated data acquisition system that is connected to REALTIME via universal serial bus (USB) cable. These recordings allow postprocessing to determine puff topography measures (eg, puff duration, volume, interpuff interval, total number of puffs) and to determine the actual fraction of smoke sampled. The output data are reported via an intuitive graphical user interface as well as in a non-proprietary (ASCII) format that allows further postprocessing by the end user.
REALTIME was validated in the clinical laboratory in an Institutional Review Board (IRB) approved study at Virginia Commonwealth University (VCU) involving 40 participants who in counterbalanced order smoked ad libitum with and without the device attached to a waterpipe, with a smoke sample fraction of 0%, 2%, 5% and 10%.26 We found no difference in puff topography, exhaled CO boost, physiological measures (heart rate and blood pressure), or subjective effects across the conditions, indicating that the device does not influence smoking behaviour or effects.
Field study
This field study was approved by the IRBs of VCU and Jordan University of Science and Technology. Participants from Irbid, Jordan were recruited into the study, at their normal places of waterpipe use. We used a convenience sample; criteria included being aged 18 years or more, being an experienced waterpipe user (regular or current waterpipe use for at least a year), and we aimed to recruit participants of both sexes in equal number. Each participant provided written informed consent before participation. Excluded were individuals who were under 18 years old or who did not carry an official ID verifying their age.
Immediately before a waterpipe use session, a brief survey form was completed indicating the session place, date, start time and participant’s age, age of smoking initiation, and frequency of waterpipe smoking. Expired-air CO concentration was measured before each session and exactly 5 min after the last puff, using a breath CO monitor (Vitalagraph, Lenaxa, Kansas, USA). Expired-air CO is highly correlated with carboxyhaemoglobin level27 and is a commonly used measure of tobacco smoke exposure.28 29 After attaching REALTIME to the participant’s waterpipe, the participant was allowed to smoke ad libitum. Participants were allowed to use their own tobacco and charcoal and to load their preferred amounts into the waterpipe, and to replace charcoal or waterpipe heads at will. Participants used their own waterpipe apparatus but used our customised hose which had the REALTIME device attached to it. All participants were compensated the Jordanian equivalent of US$20 for their time and inconvenience.
Steps for filter and DNPH cartridge sampling and storage are described in online supplementary appendix 1.
Supplementary file 1
Analytical chemistry
All analytes were determined per below procedures. Inhaled toxicant load from a given use session was reported after correction for the sampled fraction of the smoke. All solvents and standards were obtained from Sigma-Aldrich, unless otherwise stated.
Total particulate matter
TPM was determined gravimetrically as the change in weight of the filter pad. We note that TPM includes all particulate mass, including water, and is therefore not a direct quantitative measure of harmful smoke constituents. Furthermore, its chemical profile is likely to differ significantly between waterpipe and cigarette smoke.
Nicotine
Nicotine was determined by gas chromatography-mass spectrometry (GC-MS) analysis (Thermo Scientific TRACE GC-Ion Trap MS, Thermo Fisher Scientific, Waltham, Massachusetts, USA) for filter samples extracted in an ethyl-acetate solvent as described elsewhere.30 An extracted calibration curve with concentrations ranging from 1 to 20 ppm and spiked with the internal standard hexadecane was used to interpret the resulting chromatograms. This procedure results in an average recovery near 90%, and a limit of detection (LOD) of 0.5 µg.
Polycyclic aromatic hydrocarbons
Collected samples were analysed for 16 particle-bound US Environmental Protection Agency priority pollutant PAHs using a method reported previously31 with some modification. Prior to extraction, glass fibre filters were spiked with deuterated standards (acenaphthene-D10, phenanthrene-D10, chrysene-D12 and perylene-D12 procured from Absolute Standards). Then they were extracted using 8 mL toluene by 2-hour sonication followed by 30 min shaking at 250 rpm. The filters were then removed and the sample volume was reduced to 1 mL under a gentle flow of nitrogen. Subsequently, the concentrated samples were cleaned by silica solid phase extraction and concentrated again to a volume of 50 µL for GC-MS analysis. Blank filters were analysed in parallel to assess the filter background levels.
Extracted samples were analysed on a Thermo Trace GC Ultra equipped with an ITQ-900 MS detector. Chromatographic separation was carried out on a Thermo TG-5MS column (30 m×0.25 mm, 0.25 µm film thickness), using 1 mL/min helium as the carrier gas. Splitless injection volume of 1 µL was used and the injector temperature was set at 280°C. The temperature programme of the oven was as follows: 80°C for 4 min, 10°C/min to 170°C (hold for 1 min), 3°C/min to 180°C, 10°C/min to 270°C and 3°C/min to 300°C (hold for 3 min). The mass spectrometer was operated in electron impact ionisation mode with an ionising energy of 70 eV and scanning from m/z 50–350 at an ion source temperature of 250°C. Quantification was done in selected ion current profile using a calibration curve of PAH standards and deuterated PAH standards at seven different concentration ratios. The concentration of PAH standards ranged between of 0.05 and 1 ppm while that of deuterated standards was fixed at 0.6 ppm. The instrumental LOD for the 16 PAHs was found to range between 0.98 and 9.9 ng. The recovery of each PAH ranged between 65% and 128%.
Volatile aldehydes
VAs were trapped on DNPH cartridges, which were eluted with 5 mL of acetonitrile, filtered and delivered into amber vials to be analysed by high-performance liquid chromatography–mass spectrometry (LC/MSD Trap XCT, Agilent Technologies, Santa Clara, California, USA).32 Cartridges were stored at 4°C until analysis, within 2 weeks of sampling. Recoveries ranged between 90% and 102%. The species analysed, and the LOD and limit of quantification were respectively as follows (ppm): formaldehyde, 0.002 and 0.007; acetaldehyde, 0.004 and 0.012; acetone, 0.001 and 0.004; acrolein, 0.003 and 0.012; propionaldehyde, 0.008 and 0.028; crotonaldehyde, 0.005 and 0.015; methacrolein, 0.004 and 0.014; butyraldehyde, 0.006 and 0.022; benzaldehyde 0.009 and 0.029; and valeraldehyde, 0.002 and 0.007.
Carbon monoxide
CO was quantified using a calibrated electrochemical CO analyser (Monoxor II, Bacharach) that was connected to the Teflon bag after the smoking session was terminated. The CO yield mass was computed using the ideal gas law; we multiplied the measured volume concentrations by the total drawn smoke volume and the density of CO at ambient temperature and pressure to obtain the mass of CO emitted.
Statistical analysis
We reported means with 95% CIs for all variables except for CO, nicotine and benzo[a]pyrene toxicant yields, for which medians and IQRs were reported. Normality was determined by the skewness and kurtosis test for normality. We checked for differences in smoking behaviour by location of use (home or café), by sex and by smoking frequency (daily or weekly) by conducting independent samples t-tests. The correlation and regression between five selected toxicants (TPM, CO, nicotine, benzo[a]pyrene and formaldehyde) and the total inhaled volume were performed using Pearson (for TPM and formaldehyde) or Spearman’s (for CO, nicotine and benzo[a]pyrene) correlation and linear regression modelling.
Results
Of 110 approached individuals, 87 agreed to participate, although the results of 8 were discarded due to analytical error (n=6) or duplication (n=2). We, therefore, analysed users of 79 singleton waterpipe tobacco sessions: 52% (n=41) were male, the mean age was 27.0 (SD 8.1), the mean waterpipe tobacco smoking history was 4.6 (SD 3.3) years. Nearly all sessions (95%, n=75) took place at participants’ homes, whereas the remainders were conducted in cafés. Over half (54.4%, n=43) were daily users, 44.3% (n=35) were weekly users and 1.3% (n=1) was a monthly user. Averaged across all 79 sessions, the total smoking time was 46.9 min (95% CI 44.9 to 49.0), the number of puffs was 290 (95% CI 266 to 315) and the total puffing time was 15.3 min (95% CI 12.3 to 18.3). Participants inhaled an average of 214 L per session (95% CI 196.7 to 232.1), with puffs measuring approximately 0.79 L (95% CI 0.73 to 0.86) each. Puff duration and interpuff interval averaged 2.9 s (95% CI 2.7 to 3.1) and 7.6 s (95% CI 6.9 to 8.3), respectively. We found no significant differences in puff topography by location (home or café), by sex or by smoking frequency (daily or weekly) (table 1). The average expired CO increase was 45.3 ppm (95% CI 39.0 to 51.7) per person compared with baseline expired CO levels (average presession: 15.1, 95% CI 12.4 to 17.7; average postsession: 60.4, 95% CI 52.8 to 68.0).
Differences in smoke topography by location of use and by sex, mean (95% CI)
Toxicants per session
We had full session data on TPM (n=79), but due to human error or equipment malfunction one session less for CO (n=78) and nicotine/PAHs (n=37/41), and two less for VAs (n=77). Mean (95% CI) values per session were 1910 mg of TPM (1710–2100), 259 mg of CO (228–291), 5.0 mg of nicotine (4.2–5.8), 117 ng of benzo[a]pyrene (97–137) and 198 ng of formaldehyde (95% CI 175 to 220). Median (IQR) values for non-normally distributed variables were 235 mg of CO (75.8–534), 4.8 mg of nicotine (3.36–6.87) and 118 ng of benzo[a]pyrene (77.9–143). Mean values per session of other species of PAHs and VAs are available in online supplementary appendix 1.
Relationship between total inhaled volume and selected toxicants
Figure 2 presents correlations between total inhaled volume and selected toxicants. We found significant positive correlations between total inhaled volume and TPM (r=0.472; p<0.001), CO (ρ=0.746; p<0.001), nicotine (ρ=0.357; p=0.030), benzo[a]pyrene (ρ=0.340; p=0.030) and formaldehyde (r=0.526; p<0.001). For every 1 L increase in total inhaled volume, the total amount of toxicant exposure increased on average by 5.27 mg (95% CI 3.04 to 7.50, p<0.001) for TPM, 0.61 mg (95% CI 0.49 to 0.72, p<0.001) for CO, 0.31 mg (95% CI −0.06 to 0.69, p=0.10) for nicotine, 0.32 ng (95% CI −0.18 to 0.52, p=0.07) for benzo[a]pyrene and 0.66 ng (95% CI 0.42 to 0.81, p<0.001) for formaldehyde. We also found a significant positive correlation between expired CO and CO yield (r=0.421; p<0.001).

{kind=link}
{kind=link}
Toxicant yield versus inhaled volume. CO, carbon monoxide; TPM, total particulate matter.
Discussion
This study provides perhaps the strongest evidence to date that waterpipe use in the real world involves inhalation of large quantities of the major toxicants associated with addiction, pulmonary and cardiovascular disease, and cancer in tobacco cigarette smokers, and is therefore a serious public health concern. Our measurements demonstrate wide variability in puffing behaviour and toxicant inhalation that is expected in a natural setting. Despite the variability, there is a strong relationship across behaviours and products between the amount of smoke drawn and the quantity of toxicants inhaled. CO was most strongly associated with total inhaled volume, which is sourced from the burning charcoal. Furthermore, the expired CO and CO yield correlation is a valuable indicator of exposure of other toxicants, showing that these toxicants are absorbed by the smoker because they are found in the smoke.33 Reported values were obtained from a single type of waterpipe tobacco, mo’assel and with a small study population of singleton users drawn from one geographical area and mainly from one setting (homes). Other types of waterpipe tobacco, other populations, participants in other settings and those sharing the apparatus may have different puff topography and toxicant inhalation. Our sample was not intended to be representative of all waterpipe tobacco users, and that our sample’s smoking location was mainly home may mean the results are not generalisable to café settings. The external validity of this study is therefore uncertain. We did not measure concurrent cigarette use, which may act as a confounder in the smoke topography parameters and therefore toxicant exposure of users. Another important limitation is that we did not measure tobacco-specific nitrosamines, an important class of toxicants.
Two pertinent discussion points follow. The first is the extent to which previous studies of waterpipe toxicant yield, including those tightly controlling for the numerous variables in waterpipe smoking behaviour, were justified in portraying waterpipe tobacco as a public health concern. The second is understanding the extent to which our measured toxicant values are of relative concern, which can be addressed by contextualising these values against those derived from cigarette smoke. Tables 2 and 3 report on both discussion points. Table 2 shows that while our mean session length (47 min) was within range of other studies (31–64 min), our sample had the highest volume of smoke drawn (214 L), highest number of puffs (290) and shortest interpuff interval (7.6 s), than any other study on record. Table 3 shows corresponding toxicant yields from our study and the literature. Expectedly, our study’s toxicant yields are higher than all other studies with reference to TPM and formaldehyde, and second highest with respect to nicotine and CO. These high yields are likely to be due to the intensive puffing behaviour of our sample (eg, total inhaled volume per use session), the parameters for which are the highest recorded to our knowledge. Intense puffing behaviours could reflect cultural differences in waterpipe tobacco use behaviours, or that this sample was more nicotine dependent. Further research should assess the association between waterpipe smoking location and dependence. It is less plausible that researcher observation influenced puffing behaviours, which one could expect in laboratory settings, given the researchers sat a distance away from the participant and remained inconspicuous. Table 3 also shows that relative to the toxicant exposure from a single cigarette, the smoke of one waterpipe session contains substantially higher yields of nicotine and CO (between 2 and 50 times that of a cigarette), and similar yields of the carcinogens benzo[a]pyrene and formaldehyde.17
Comparison of measured puff topography with previous studies (parenthesis indicate 95% CIs unless otherwise stated)
Comparison of measured toxicant content with previous studies (parenthesis indicate 95% CIs unless otherwise stated)
A strength of this study is that it is the first to our knowledge to measure directly PAHs and VAs in the natural setting. The data that we report confirm previous observations from controlled laboratory studies17 and add to the growing body of literature that action is needed to reduce population harm from waterpipe tobacco.34 We are also the first to measure toxicant exposure in a home setting, which could add a new angle to the discussion around waterpipe should further research identify, for example, that home users are more dependent on waterpipe tobacco than café users.
To conclude, singleton waterpipe tobacco users in Jordan engaging in ad libitum smoking, most of whom were in their homes, demonstrate a harmful toxicological profile that appears more substantial than that found in the existing literature. We further demonstrated that toxicants found in trace quantities, such as benzo[a]pyrene and formaldehyde, are present in quantities that warrant public health concern. Further research could evaluate how patterns of use vary across settings and between sociodemographic groups.
What this paper adds
Studies have shown that waterpipe tobacco likely has a harmful toxicological profile. However, waterpipe toxicant inhalation estimates are limited to controlled experiments involving numerous idealisations.
The degree to which toxicant inhalation with real-world waterpipe use is represented by controlled laboratory studies is not known, providing aficionados and marketers space to sow doubt about its harmful effects.
We present waterpipe toxicant data from ad libitum waterpipe smokers in their natural environment using a real-time in situ device. We demonstrate a substantial toxicological profile, possibly the highest on record, in this population. We demonstrate for the first time that real-world waterpipe use involves inhalation exposure to substantial quantities of carcinogens and lung irritants.
This study provides perhaps the strongest evidence to date that waterpipe use in the real world involves inhalation of large quantities of the major toxicants associated with addiction, pulmonary and cardiovascular disease, and cancer in tobacco cigarette smokers, and is therefore a serious public health concern.
References
Footnotes
Contributors Study conception and design: AS and TE. Acquisition of data: AS, KHA, OFK, RB, RE-H, RS, NK and TE. Analysis and interpretation of data: AS, EKS, KHA, MJ, OFK, RE-H, RS and TE. Drafting of manuscript: AS, KHA, MJ, OFK, RS and TE. Critical revision: AS, EKS, KHA, MJ, NAS, NK, OFK, RB, RE-H, RS and TE.
Funding This study was funded by NIH/NIDA grant number R01 DA025659. TE, Saliba, EKS and AS currently are supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number P50DA036105 and the Center for Tobacco Products of the US Food and Drug Administration.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the views of the NIH or the FDA.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.