Article Text

Abstract
Introduction England introduced a tobacco display ban for shops with >280 m2 floor area (‘partial ban’) in 2012, then a total ban in 2015. This study assessed whether these were linked to child awareness of and access to cigarettes.
Methods Data come from the Smoking, Drinking and Drug Use survey, an annual survey of children aged 11–15 years for 2010–2014 and 2016. Multivariate logistic regression models assessed changes in having seen cigarettes on display, usual sources and ease of access to cigarettes in shops
Results During the partial display ban in 2012, 89.9% of children reported seeing cigarettes on display in the last year, which was reduced to 86.0% in 2016 after the total ban (adjusted OR 0.58, 95% CI 0.50 to 0.66). Reductions were similar in small shops (84.1% to 79.3%)%) and supermarkets (62.6% to 57.3%)%). Although the ban was associated with a reduction in the proportion of regular child smokers reporting that they bought cigarettes in shops (57.0% in 2010 to 39.8% in 2016), we did not find evidence of changes in perceived difficulty or being refused sale among those who still did.
Discussion Tobacco point-of-sale display bans in England reduced the exposure of children to cigarettes in shops and coincided with a decrease in buying cigarettes in shops. However, children do not report increased difficulty in obtaining cigarettes from shops, highlighting the need for additional measures to tackle tobacco advertising, stronger enforcement of existing laws and measures such as licencing for tobacco retailers.
- advertising and promotion
- prevention
- public policy
Statistics from Altmetric.com
Background
Most people who smoke start smoking during childhood.1 This means that measures to reduce child uptake of smoking are essential to bring the tobacco epidemic to an end, delivering the objective of a ‘smoke free generation’. One such strategy is the introduction of point-of-sale display bans to reduce the visibility and appeal of tobacco products. There is evidence that exposure to retail tobacco displays increases desire to smoke and to make unplanned purchases while reducing the likelihood of making a successful quit attempt.2–5 Children are particularly susceptible to tobacco marketing that can influence their behaviour as well as altering their perception of the acceptability of smoking and estimates of peer smoking rates.6–8
The WHO MPOWER strategy includes ‘Enforce bans on tobacco advertising, promotion and sponsorship’ as one of its six pillars, and Article 13 of the WHO Framework Convention on Tobacco Control, which came into force in 2005, advocates a complete ban on any display of tobacco products at points of sale.9 Tobacco display bans are popular,10 but policies in this area face pushback from the tobacco industry and its proxies,11 so data evaluating their impact should form a useful guide for legislators considering implementing this policy. Ecological data from countries that have implemented such bans have found them to be linked to declines in adult smoking prevalence, as has individual-level data on the impacts of banning the display of cigarettes from large shops in England.12 13 Available analyses so far, however, have not considered the impacts of the policy on children.
A ban on the display of tobacco products was introduced in England for large shops (>280 m2 floor area) from 6 April 2012 and this was extended to all shops on s6 April 2015.14 15 We used data from the annual English Smoking, Drinking and Drug Use (SDDU) survey of children to assess whether there had been a change in children’s exposure to cigarette packets, where children who smoked are obtaining cigarettes and ease of accessing cigarettes in shops.
Methods
Data for this study come from the SDDU survey for England, which is used by the government to monitor performance of the Tobacco Control Plan in terms of youth smoking.16 17 The survey includes schoolchildren in years 7–11 (mostly aged 11–15 years) with data collected by a self-completion paper questionnaire during school time in ‘exam conditions’ with pupils unable to discuss questions or look at each other’s answers. The survey is designed to be representative of the sex, school year and region of children in England with schools selected to provide a mixture of school types (comprehensive, secondary modern, grammar, private, single sex and mixed), by each region of England. Survey sampling was between September and January for each year, and thus the 2012 data are from at least 5 months after the introduction of the partial ban, and the 2016 data are from at least 15 months after the introduction of the total ban. The timings of data collections in relation to the policy changes are displayed in figure 1.

Data collection points and tobacco display ban policy changes.
SDDU is cross-sectional with no repeated measures on the same children, with sample sizes for each year ranging from 6173 (2014) to 12 051 (2016). We used complete case analysis, and as the different outcomes were asked in different years, there were differing sample sizes for each analyses. Numbers of respondents in each analysis are detailed in the appropriate tables.
Variables
This study investigated a number of outcomes that were assessed as follows. Exposure to cigarette packaging was assessed in 2012, 2014 and 2016 using the question, ‘In the past year, have you seen cigarette packets on display in any of the shops listed below? Only include shops where you have seen cigarette packets displayed on a shelf or counter. Do not include signs or adverts saying cigarettes can be bought.’. Children could tick all responses that applied, and answers were: a supermarket; a newsagent, tobacconist or a sweet shop; a petrol station or garage shop; and some other type of shop.
Sources of cigarettes were assessed in 2010, 2012, 2014 and 2016 using the question, ‘Where do you usually get your cigarettes from?’. Children could tick more than one box from a possible 14 responses. We grouped these into buying from shops (supermarkets, newsagents, garages or ‘some other type of shop’), buying from other sources (buying from friends, machines, the internet or street markets) and being given cigarettes (by friends, parents, siblings or ‘someone else’). We also additionally investigate buying from small shops, buying from large shops (supermarkets) and buying from friends individually.
We used two measures of ease of access to cigarettes in shops collected in 2010, 2012, 2014 and 2016. First, being refused sale of cigarettes in a shop was assessed using the question, ‘The last time you went into a shop to buy cigarettes, what happened?’ with possible responses, ‘I bought cigarettes’ and ‘the shopkeeper refused to sell me cigarettes’. Second, reported difficulty in obtaining cigarettes in shops was assessed using the question, ‘On the whole, do you find it easy or difficult to buy cigarettes from a shop?’, which was categorised into ‘fairly or very easy’ versus ‘very or fairly difficult’.
The SDDU collects other data from children that we have included as potential confounders of the main relationships of interest. These were age, sex, ever use of alcohol (yes/no) and ever use of drugs (yes/no). We also use data on the smoking status of children. In line with the official SDDU reports, we categorise this into non-smokers, occasional smokers (children reported smoking fewer than one cigarette a week) and regular smokers (smoking at least one cigarette a week).16
Analyses
All outcomes were first explored descriptively. Logistic regression models assessed whether levels of exposure to cigarette packaging in 2014 and 2016 were different to those in 2012 after controlling for age, sex, ever use of drugs, ever use of alcohol and smoking status. These models were performed separately for small shops and large shops, then exposure in any shop. We also present subgroup analyses of changes in exposure in any shop stratified by each of our age, sex, alcohol use, drug use and smoking status subgroups. In order to investigate potential differences in changes across groups, interaction tests were used to assess the statistical significance of changes between 2016 and 2012 across each subgroup of age, sex, ever use of alcohol and drugs and smoking status studied.
In order to assess changes in usual source of cigarettes among regular smokers, we first ran logistic regression models assessing differences in buying in shops, buying from other sources and being given cigarettes. Then, to assess potential differences due to the legislation targeting first large and then small shops, we used three separate models for each of small shops, large shops (supermarkets) and in buying cigarettes from friends. These models used 2010 (before any display bans) as a reference and controlled for age, sex, ever use of alcohol and ever use of drugs. The primary analyses for all of these outcomes are based only on children categorised as regular smokers. We additionally present these same analyses in the appendix based on both regular and occasional smokers. We used the same modelling strategy to examine our two measures of ease of access to cigarettes in shops. All regression analyses employed survey weights derived by the SDDU team to correct for unequal probabilities of selection between sex, school year and regions.
Results
A percentage of 89.9 of children reported being exposed to cigarette packaging in shops in 2012, which increased to 92.6% in 2014 (adjusted OR (AOR) 1.26, 95% CI 1.10 to 1.44 and decreased to 86.0% in 2016 (AOR 0.58, 95% CI 0.50 to 0.66) (table 1). A similar trend was observed for small shops: 84.1% of children were exposed in 2012, 86.1% in 2014 (AOR 1.11, 95% CI 1.00 to 1.24) and 79.3% in 2016 (AOR 0.65, 95% CI 0.58 to 0.73). For large shops there were declines in exposure from 62.6% in 2012 to 61.1% in 2014 (AOR 0.89, 95% CI 0.83 to 0.96) and 57.3% in 2016 (AOR 0.70, 95% CI 0.64 to 0.77).
Changes in children’s exposure to cigarette packaging in shops in 2012–2016
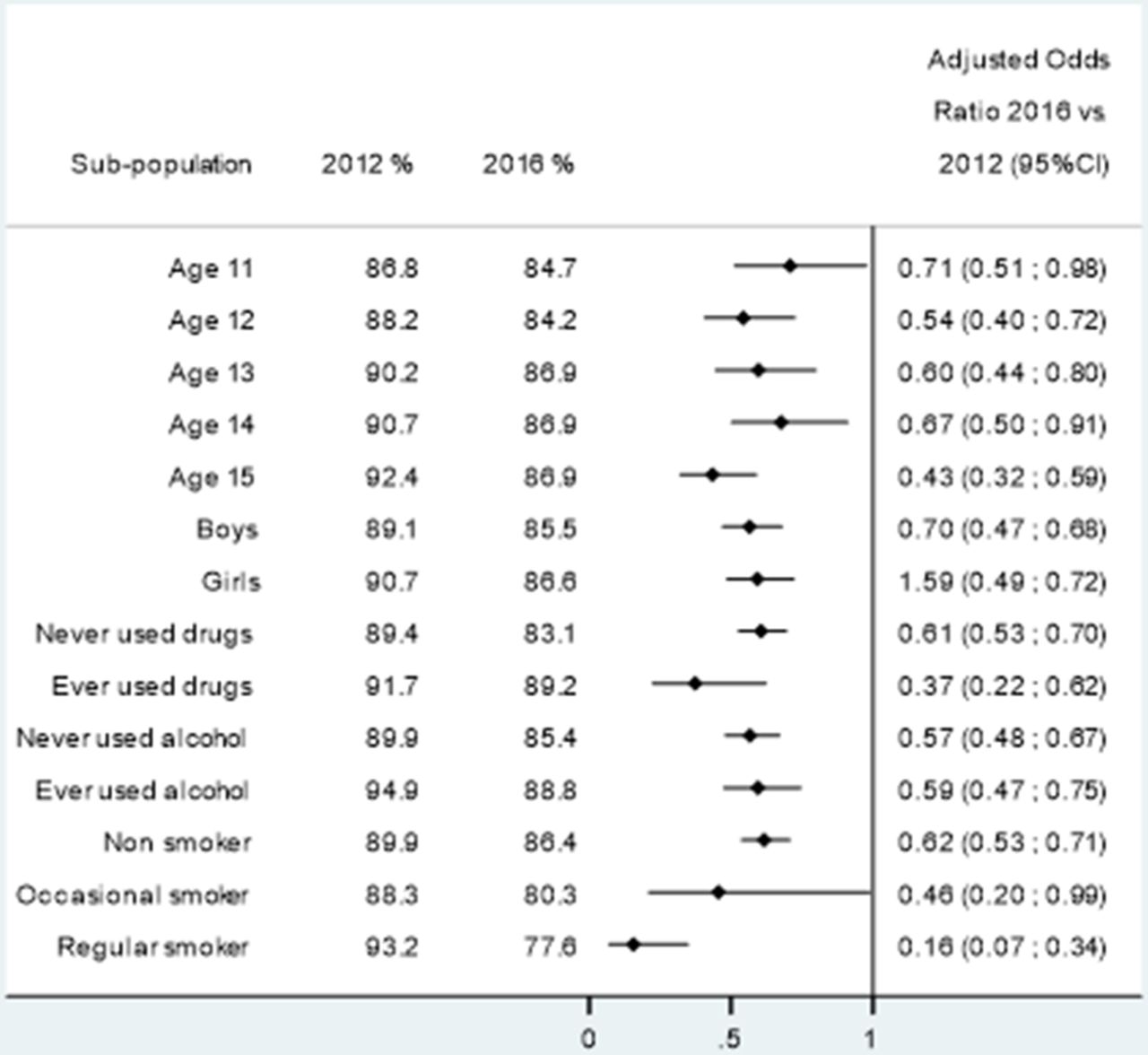
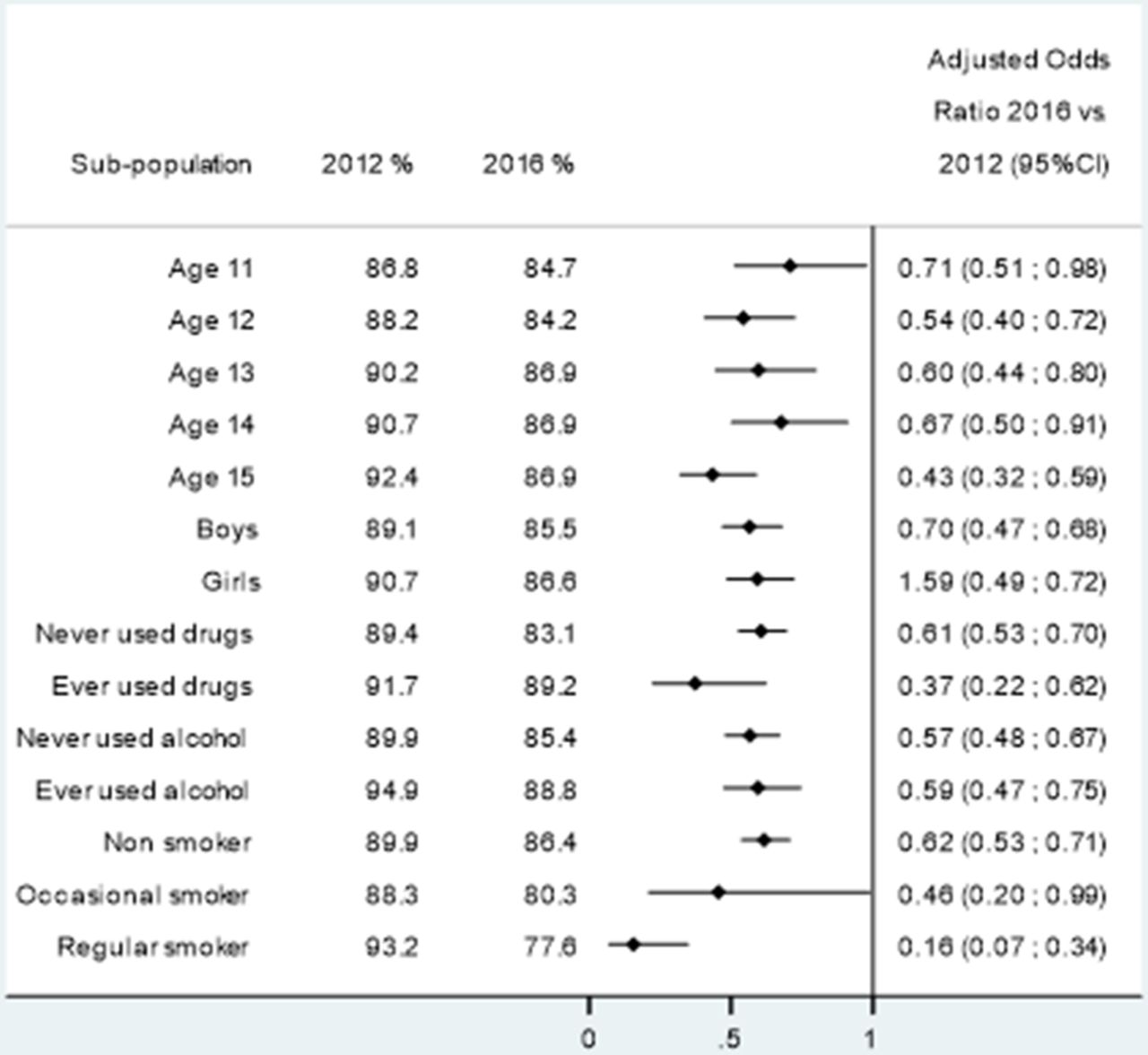
All of the groups we studied experienced statistically significant declines in exposure to cigarette packaging in shops over the study period (figure 2). Interaction testing of changes between 2012 and 2016 for different groups find that there were larger reductions among individuals aged 15 years than individuals aged 11 years, from −2.1% for individuals aged 11 years to −5.5% for individuals aged 15 years (p value for difference=0.033; supplementary appendix table A1). There were also larger reductions among regular smokers (−15.6%) than among non-smokers (−3.5%, p value for difference=0.001).
Supplementary file 1
{kind=link}
{kind=link}
Changes in exposure to cigarettes in shops 2016 versus 2012.
Buying from a shop was a usual source of cigarettes for 57.0% of the sample regular child smokers in 2010, and this was not significantly different in 2012 or 2014. In 2016, this declined to 39.8% (AOR 0.42, 95% CI 0.25 to 0.70) (table 2). Buying from sources other than a shop was a usual source for 39.3% of regular child smokers in 2010, which declined to 28.0% in 2014 (AOR 0.62, 95% CI 0.41 to 0.93) and 26.1% in 2016 (AOR 0.41, 95% CI 0.24 to 0.70). Being given cigarettes was a usual source for 62.4% of regular child smokers in 2010, and this did not change over the study period, for example, 60.9% in 2016 (AOR 0.81, 95% CI 0.48 to 1.38).
Changes in usual sources of cigarettes among regular child smokers in 2010–2016
A percentage of 51.1 of regular child smokers noted small shops as a usual source of cigarettes in 2010, which was unchanged in 2012 and 2014 but declined to 34.2% in 2016 (AOR 0.31, 95% CI 0.18 to 0.51). A percentage of 14.9 of regular child smokers used supermarkets as a usual source for cigarettes in 2010, and this was not found to change statistically significantly during the study period. A percentage of 34.3 of children reported that buying cigarettes from friends was a usual source of cigarettes in 2010, which declined to 25.5% in 2016 (AOR 0.50, 95% CI 0.29 0.83)
Unweighted percentages show that the most common source of cigarettes in 2010 was being given by friends, followed by buying from a newsagent and that there was relatively little change in these rankings between 2010 and 2016 (online supplementary appendix table A2). Logistic regression analyses of changes in sources of cigarettes over time among both regular and occasional smokers give similar results to our main analyses among regular smokers only (online supplementary appendix table A3)
A percentage of 31.2 of regular child smokers reported being refused the sale of cigarettes at their last attempt, and this was not found to be statistically significantly different in any of the later years (table 3). For example, 32.5% of regular child smokers reported being refused in 2016 (AOR 1.23, 95% CI 0.58 to 2.66). A percentage of 61.0 of children reported that it was easy or very easy to buy cigarettes in shops in 2010, which also was not found to be statistically significantly different in any of the later years. For example, 64.7% of regular child smokers reported that cigarettes were easy or very easy to buy in 2016 (AOR 0.60, 95% CI 0.31 to 1.13).
Changes in perceived ease of buying cigarettes in shops among regular child smokers in 2010–2016
Sensitivity analyses of both of these outcomes among both regular and occasional smokers do not suggest any changes in ease of accessing cigarettes in shops for children attempting to buy them in shops (online supplementary appendix table A4).
Discussion
The main findings of this study are that: (1) the tobacco display ban was associated with a reduction in children’s exposure to tobacco packaging in shops; (2) there was a substantial reduction in children who smoked obtaining cigarettes from shops; and (3) we did not find evidence of changes in the perceived difficulty of obtaining cigarettes among children who did buy them from shops.
The present data suggest that there was a modest fall in the proportion of children reporting exposure to cigarette packaging in shops following the partial and complete bans on tobacco displays. Since tobacco displays stimulate the desire to smoke, a reduction in their visibility to children is welcome and suggests that the ban is working as intended. The reduction in exposure was found to be consistent between sexes but with potentially larger associations among individuals aged 15 years than individuals aged 11 years. The reduction in reports of having seen cigarettes in shops was greatest in those who were regular smokers (93.2% in 2012 to 77.6% in 2016 following the total ban), who may be more accurate in their recall of tobacco packaging display. The findings are consistent with Australian data on the effectiveness of tobacco control policies that suggests a significant link between the extent of implementation of point of sale and outdoor advertising and adolescent smoking rates.18 Our findings do suggest, however, that the majority of children still report seeing cigarettes in the previous year, which is consistent with international evidence on tobacco display bans, where large numbers of people still report seeing cigarettes on display despite official reports of compliance being high.19 20 In England, a 2016/2017 report by Trading Standards, which enforces tobacco promotion and sale legislation on behalf of the Department of Health, found that there was 92% compliance with tobacco display bans in England.21 Even perfect compliance with the display ban will still provide some opportunities for children to see cigarettes packaging if they are waiting to be served when the display cabinet is opened for another customer. However, the exact mechanism then by which so many children report seeing cigarettes on display deserves further investigation and may suggest that more rigorous assessments of compliance would be beneficial, especially in order to assess whether any impacts of the display ban changes over time. Nonetheless, display bans can also be effective in reducing smoking behaviour as part of general efforts to denormalise tobacco use, as well as communicating negative perceptions of society as a whole to tobacco use.19
The survey period also show changes over time in where children who are regular smokers obtain cigarettes. The most common method of obtaining cigarettes remains being given them by friends and fewer children now report that they buy cigarettes themselves. These data also reinforce the important role of small shops such as newsagents and garages in allowing children to obtain cigarettes, which is now becoming less common. For example, there were substantial falls in the proportion of regular smokers reporting that they bought them from newsagents (46.1% 2010 to 30.4% 2016) or garages (15.4% to 6.8%)%). In all forms of shops, the additional need for tobacco displays to be opened may act as a psychological deterrent for some children or may serve as a reminder to people working in shops that they are selling a product that has age restrictions. However, during the time period studied here, there have been substantial falls in funding for enforcement of age of sale and other tobacco sale restrictions; – there has been a 56% reduction in full-time equivalent Trading Standards staff in England between 2009 and 2016.22 Local directors of public health have also expressed concerns about levels of funding available for the enforcement of such legislation among other policies such as smoking cessation.23 International evidence is clear that even modest investments in enforcement of existing laws has an impact on sales to minors, and additionally that enforcement can assist with the effectiveness of other policies to reduce smoking among youth and in adults.24–27 Together these findings suggest that the legislation is having some success despite these falls in enforcement spending and that greater reductions could be achieved if this spending was increased. They also suggest that a tobacco retailer scheme may be required if access to cigarettes among children is to be fully controlled.28 Finally, while data limitations means we were unable to examine the issue here, existing evidence also suggests that enforcement of age of sale laws has impacts on smoking that are similar across markers of socioeconomic circumstances.29 30
Displays of cigarettes at the point of sale are only one method among many by which tobacco is advertised, which includes in social media and on cigarette packets. Point-of-sale display bans are thus an important intervention to reduce the exposure of populations to tobacco advertising, but a comprehensive approach is needed. For example, interventions to either remove protobacco messages or promote antismoking are both effective at reducing smoking levels.31 32 Both antismoking advertising intensity and duration are important for ensuring reductions in adolescent smoking prevalence and must receive an appropriate level of funding.33 34 More recently, some countries, including the UK, have moved to restrict the potential for tobacco to be advertised on cigarette packets by implementing standardised packaging for tobacco, which is reducing smoking levels.35–37 The increasing influence of social media as a vehicle for advertising cigarettes has also been noted, and this may need additional legislation.38
Strengths and limitations
This study presents the first national analysis of the impacts of banning tobacco displays at the point of sale in England on children’s exposure and access to tobacco products. It relies on data used by the government to monitor smoking prevalence among children and allowed consideration of data from a number of years. However, there are some limitations to consider. During the study period, there has been both a secular fall in smoking prevalence as well as other changes in legislation, such as the ban on cigarette vending machines, publicity around standardised packaging and bans on smoking in cars with children as well as steady increases in the price of cigarettes. Nonetheless, the SDDU does reflect the behaviours, experience and attitudes of children who continue to smoke in England. The period covered (2010– 2016) also includes the emergence of e-cigarettes into the UK market. The 2016 SDDU asked children about e-cigarettes and found that regular use was 2% in 2016, and in line with other data found that the majority of use was among current tobacco users.39 40 Similar to cigarettes, the most common sources of e-cigarettes were being given by friends (35% of regular users), although other common methods of obtaining them included buying from an e-cigarette shop (24% of regular users) and buying from the internet (23% of regular users). While positive for health, the declining rate of smoking among young people does mean that our analyses of sources of cigarettes and ease of access among regular smokers are based on small sample sizes. In line with the official reports from SDDU, we restrict our main analyses on sources of cigarettes to regular child smokers, the numbers of which have been declining over this time period, which could lead to an underestimate of the impact of the display ban. However, we have tried to limit these problems by including sensitivity analyses from the larger group of current smokers, which gave similar results to our main findings. It is also possible that point-of-sale display bans have played a direct role in this fall in prevalence, with those who find it more difficult to obtain cigarettes either quitting smoking or not becoming smokers, but we have no data to address this directly.
The SDDU survey contains limited covariate data that restricts our ability to control for potentially important confounders that may influence exposure to tobacco or the sources children who smoke make use of. Particularly, for 2016, the survey did not ask children about their eligibility for free school meals, which is a good marker of deprivation and has been used in previous research.41 42 This omission means that we cannot assess whether the total display ban had an impact on inequalities in our outcomes nor whether deprivation may have affected our estimates of effect size as factors such as smoking among friends and family are linked to socioeconomic status. Additionally, questions on the display of cigarettes were only added to the SDDU from 2012, which means we were unable to assess the levels of this exposure before the introduction of the partial point-of-sale display ban as well as whether any impacts have changed due to the introduction of the partial ban. Also, the questions covered seeing cigarettes on display in the previous 12 months, which may introduce some inaccuracy to reporting, although our data from 2016 are a full 15 months after the introduction of the total ban on cigarette display in shops. Other potential source of inaccuracy for the analyses of exposure to cigarette packaging include the long time period assessed by our exposure question (12 months) and children remembering signs such as ‘we sell cigarettes here’ or advertisements for e-cigarettes.
Conclusion
The introduction of point-of-sale display bans for tobacco products has been associated with a reduction in children’s exposure to tobacco products in shops. It has also coincided with a substantial reduction in the proportion of children buying tobacco in shops, though those who continue to do this do not appear to be finding it more difficult. Point-of-sale display bans have a role in reducing child access to tobacco, but additional measures, in particular enforcement of age restrictions on purchase and schemes to license retailers, are likely to be needed to further reduce child uptake of smoking.
What this paper adds
This study of nationally representative data for England provides the first assessment of the impacts of the tobacco display ban on children as well as detailed data on the extent of child exposure to tobacco packaging in shops and their sources of buying cigarettes.
We find that tobacco point-of-sale display bans may have a role in reducing child smoking, being associated with a reduction in exposure in shops and a reduction in buying from shops. Nonetheless, levels of exposure to cigarettes in shops remains high, and those who continue to buy from shops do not appear to be finding it more difficult.
References
Footnotes
Contributors AAL had full access to all of the data and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design was by AAL, EPV, KC-MC and NSH. All authors were involved in the interpretation of data, drafting of the manuscript and revising it for critical intellectual content.
Funding There was no specific funding for this work but CM, AAL and KC-MC are funded by the National Institute for Health Research (NIHR) (NIHR RP 014-04-032) and the Public Health Policy Evaluation Unit at Imperial College London is grateful for the support of the NIHR School of Public Health Research.
Competing interests None decalred.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement SDDU data are available free of charge to UK-based researchers through the UK Data Archive (http://www.data-archive.ac.uk/).