Article Text

Abstract
Background Philip Morris International, one of the largest transnational cigarette manufacturers, has heavily invested in its new heated tobacco product, IQOS, marketing it aggressively as a less harmful alternative to cigarette smoking. The company’s assertions that the product replaces cigarettes in a market have never been independently tested. The objective of this study is to determine whether introduction of IQOS affected cigarette sales in a large economy.
Data and Methods Using 2014 to 2018 monthly retailer panel data from Japan, we analyse whether different dates of IQOS introduction across Japan’s regions are reflected in the patterns of cigarette sales in those regions. A series of placebo models are estimated to test if events other than IQOS introduction could have better explained the observed trends in cigarette sales.
Results Cigarette sales begin to substantially decline at the time of the introduction of IQOS in each of 11 Japanese regions (Chow tests p<0.001). IQOS introduction, which varied across regions, better predicted the timing of cigarette sales decline than any one time applied to all regions simultaneously (a national-level exogenous shock) and than nearly all possible rearrangements of the true IQOS introduction months among the regions (exact permutation test’s p value from 0.02 to 0.13, depending on the study approach).
Conclusions The introduction of IQOS likely reduced cigarette sales in Japan. The net population health impact, however, cannot be assessed without resolving several key uncertainties related to the direct harms of IQOS and the precise patterns of both smoking and IQOS use.
- electronic nicotine delivery devices
- economics
- global health
- heated tobacco products
Statistics from Altmetric.com
Introduction
The introduction of novel tobacco products is shifting the composition of the tobacco and nicotine marketplace, markedly in some places. Evaluating the public health implications of these shifts is complex because new products are often claimed to be less harmful than traditional products, particularly tobacco cigarettes, but the actual harmfulness cannot be precisely determined for years or even decades. While many studies and reports observe changes in prevalence for different product classes, there has been little rigorous analysis of how the introduction of these new products affects sales of existing popular products, especially cigarettes. Such analysis could help policymakers comprehensively evaluate the impact of novel products in this volatile time.
Heated tobacco products (HTPs) are the latest in a line of products marketed as less harmful than regular cigarettes. Unlike regular cigarettes, which combust tobacco leaves, HTPs heat a processed tobacco leaf substance at a high temperature slightly short of combustion. Unlike e-cigarettes, which aerosolise a liquid containing varying amounts of nicotine (or no nicotine at all), HTPs release the nicotine directly from tobacco leaf. The product has begun to show substantial sales growth in several countries where they have been introduced. Available in more than 44 countries as of the first quarter of 2019,1 growth has been especially strong in Japan and Korea.2 3 The global HTP market leader is IQOS from Philip Morris International (PMI), which the company claims to generate a significantly lower quantity of “harmful or potentially harmful chemicals” compared with combustible cigarettes.4 PMI recently filed an application with the US Food and Drug Administration to commercialise the product in the USA.5 The application was recently approved.6 The company predicts that by 2025 their “reduced-risk” category, which could be led by HTPs, will account for over 30% of the company’s sales volume and over 38% of the company’s total net revenues globally.7 In New Zealand, PMI announced that it planned to switch its attention from cigarettes to IQOS and that it foresaw abandoning cigarette sales altogether,8 though the credibility of these claims is uncertain particularly because of its longstanding and nearly complete reliance on combustible tobacco products as the core of its business.
One of the main promises made by PMI is that IQOS is intended to displace sales of regular cigarettes. In numerous statements, the company asserts that IQOS is a “unique alternative to smoking combustible cigarettes for adult smokers”4 and that the goal of the product is “to switch hundreds of millions of adult smokers to less harmful alternatives than continued smoking as quickly as possible”.9 It is often presumed that the introduction and growth of IQOS would lead to declines in cigarette sales, but it can be difficult to find evidence for this, in part because HTPs are a relatively small part of the overall tobacco market in most places. However, in Japan, HTP sales have grown to the point where they now constitute a substantial share of the overall tobacco and vapour product market (15.5% by the PMI’s own account),7 outpacing the combined HTP and vapour product sales in any other market in total value terms entering 2018.10
This study examines whether the introduction of IQOS has causally reduced per capita cigarette sales in Japan. It utilises a natural experiment in IQOS availability created during the rollout of IQOS in 2015 and 2016. PMI first introduced IQOS to 12 prefectures in September 2015 ahead of their nationwide launch in April of 2016. This staggered rollout created exogenous variation in the availability of IQOS across regions that can be used to assess whether IQOS introduction had a causal impact on tobacco cigarette sales.
Methods
Data
Data on cigarette and heated tobacco unit sales were obtained from Intage Inc., a market research company based in Japan. The company collects data on sales of tobacco products from participating supermarkets and convenience stores and provides tobacco market size estimates for 11 of Japan’s 12 geographical regions, covering 99% of the population (Okinawa prefecture is the only region excluded from the company’s retailer panel for tobacco products). The obtained data cover the period from September 2014 to August 2018. The total number of observations in this study is 528 (11 regions x 48 months).
The Intage retailer panel data are aggregate monthly data on the number and value of items sold. While the data on cigarettes reflect sales of all cigarette brands combined, the HTP data include separate data for PMI’s IQOS. These data contain detailed information on the heated tobacco units only (PMI’s heat sticks) and does not include information on the battery-powered devices (such as the PMI’s IQOS holder) into which the heat sticks are inserted.
To construct per capita cigarette sales and per capita heat sticks sales, we use information on the total population by prefecture obtained from the Japan Statistical Office.11 The prefecture-level data were collapsed to the 11 regions in the Intage data. Because the statistical office provides population estimates as of the 1st of October each year, the data for the other months were imputed using linear interpolation.
Primary independent variable
The primary exogenous variable is derived from PMI’s timeline of IQOS introduction to the Japanese market, drawn from PMI’s documents.4 PMI started testing the product in selected stores in the city of Nagoya in November 2014.2 4 The product was then introduced to the market in two phases: the first 12 prefectures in September 2015 (treatment group) and the remaining 35 prefectures in April 2016 (control group) (see table 1 for the months of IQOS introduction by prefecture).2 4 The Intage data used in this study include regions that are generally larger than a single prefecture. Therefore, we used three approaches to assign the introduction date to each of our regions. In the first approach, we weighted the prefecture-level introduction date by the prefecture’s population. Specifically, in regions where most residents lived in prefectures with a September 2015 IQOS introduction, the assigned market introduction date was September 2015. Otherwise, the assigned market introduction date was April 2016. In the second approach, the regions that were not fully covered by IQOS rollout in September 2015 were assigned an April 2016 introduction date. Finally, in the third approach, we removed the regions with a partial September 2015 introduction from the analysis, leaving only the regions with a full September 2015 introduction and a full April 2016 introduction (table 1 lists introduction dates by region in all three approaches).
IQOS Introduction by region
Statistical method
Linear trends were fitted to the per capita cigarette sales by each region using a fixed-effects model. The region fixed effects control for different initial levels of cigarette sales in the regions, resulting from such factors as the social acceptability of cigarette use or the level of implementation of tobacco control regulations. If the link between IQOS and regular cigarette use exists, the event of IQOS market introduction will be reflected in the patterns of cigarette use. We used the “changing growth” time-trend model12 and Chow test13 to examine whether cigarette sales followed the same trends before and after IQOS introduction in Japan. The null hypothesis in the test is that the trend in per capita cigarette sales remained stable over time. The alternative hypothesis is that there was a structural break in the trends with the IQOS heated tobacco product introduction in each region, that is, that the trend lines were demonstrably kinked in the months of IQOS introduction.
Even if the Chow test finds that the trends in cigarette sales in Japan were not stable over time, this change in trends could have been caused by factors other than IQOS heated tobacco product introduction. To check for that possibility, we devised a series of placebo tests to rigorously examine the likelihood that the observed relationship between IQOS introduction and cigarette sales decline could be attributed to (1) national-level factors coinciding with IQOS introduction or (2) random chance.
First, we note that a structural break in trends in cigarette sales could have been caused by a national-level factor that affected trends in cigarette sales across all regions at once. Such a factor could include a sudden downturn in the economy, an introduction of a national-level tobacco control law or a large-scale natural disaster or any other exogenous shock. To test for this possibility, we estimated a set of placebo models explaining cigarette sales by a linear trend, each model with a kink for a different month of our analysis. We then compare the models’ ordinary R2 to those for the model in which the sales trend lines are kinked in the actual months of IQOS introduction.
To gain confidence that the association between IQOS introduction and cigarette sales decline is not due to chance, we also employed an exact permutation test. The set of actual observed IQOS introduction times was repeatedly redistributed so that one or more regions were assigned the IQOS introduction date that was originally associated with a different region. The time-trend model with the new combination of the introduction dates was then estimated and the R2 recorded. This procedure was repeated for all 330 possible unique groupings of the true, original introduction dates in Approach 1, for all 55 possible combinations in Approach 2 and for all 15 possible combinations in Approach 3. This reassignment process allowed for the creation of a null distribution of R2 values, each associated with a different reassignment of introduction dates. Under the null hypothesis that the timing of each region’s decline in cigarette sales was unrelated to IQOS introduction, the R2 value of the true introduction dates would represent a random draw from this null distribution. The placement of the model based on the actual dates of IQOS introduction within this distribution – that is, the ranking of the R2 for the introduction date model among those of the placebo permutation models – allows us to infer a p value representing the probability that an association at least as strong as the one actually observed would have occurred due to random chance.
Introduction date model and placebo models were estimated using each of the three approaches to assign IQOS introduction date to the regions where IQOS was only partially introduced in September of 2015.
Results
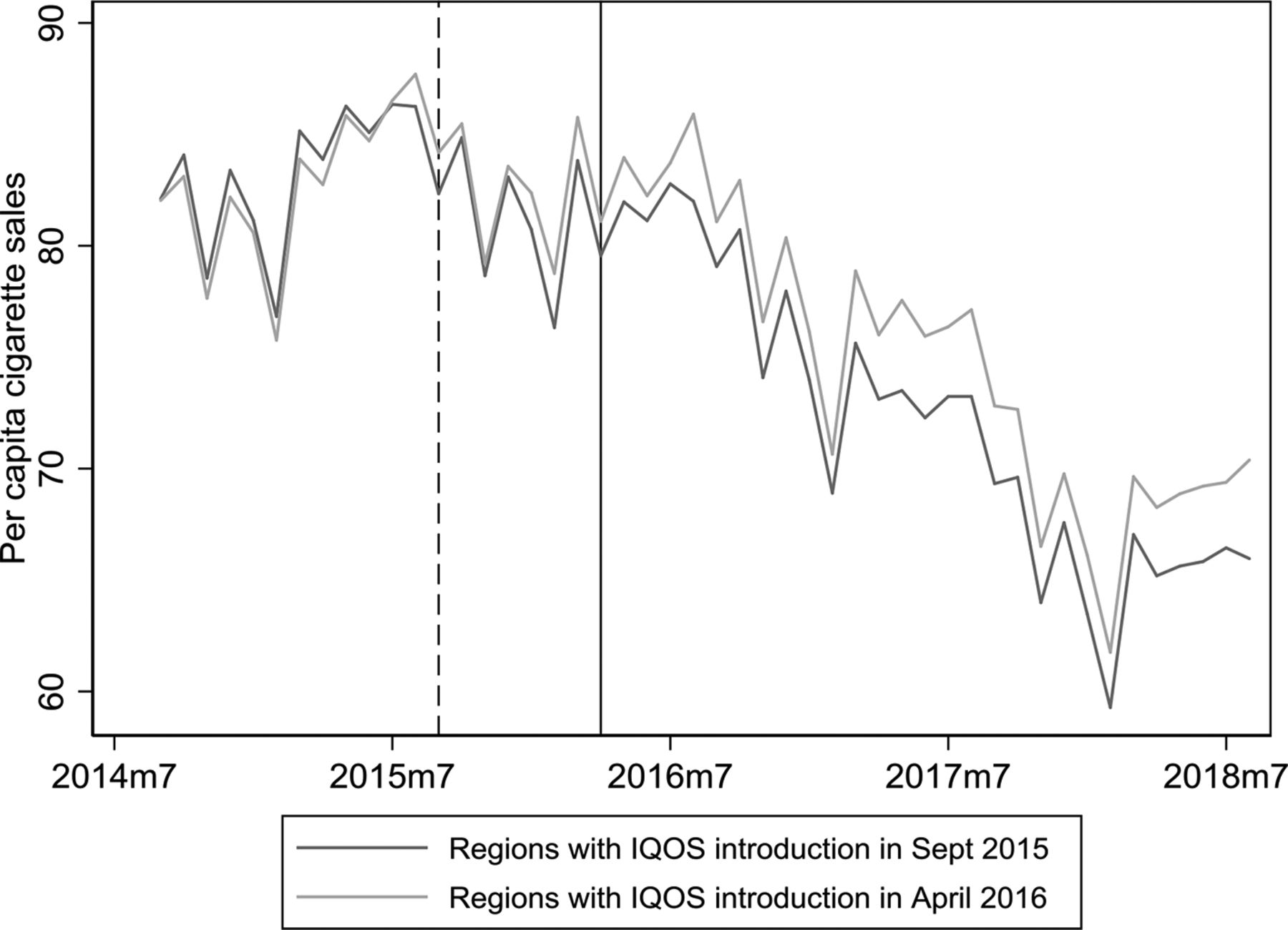
Per capita cigarette sales started to decline earlier in regions with IQOS introduction in September 2015, compared with regions with IQOS introduction in April 2016 (figure 1).
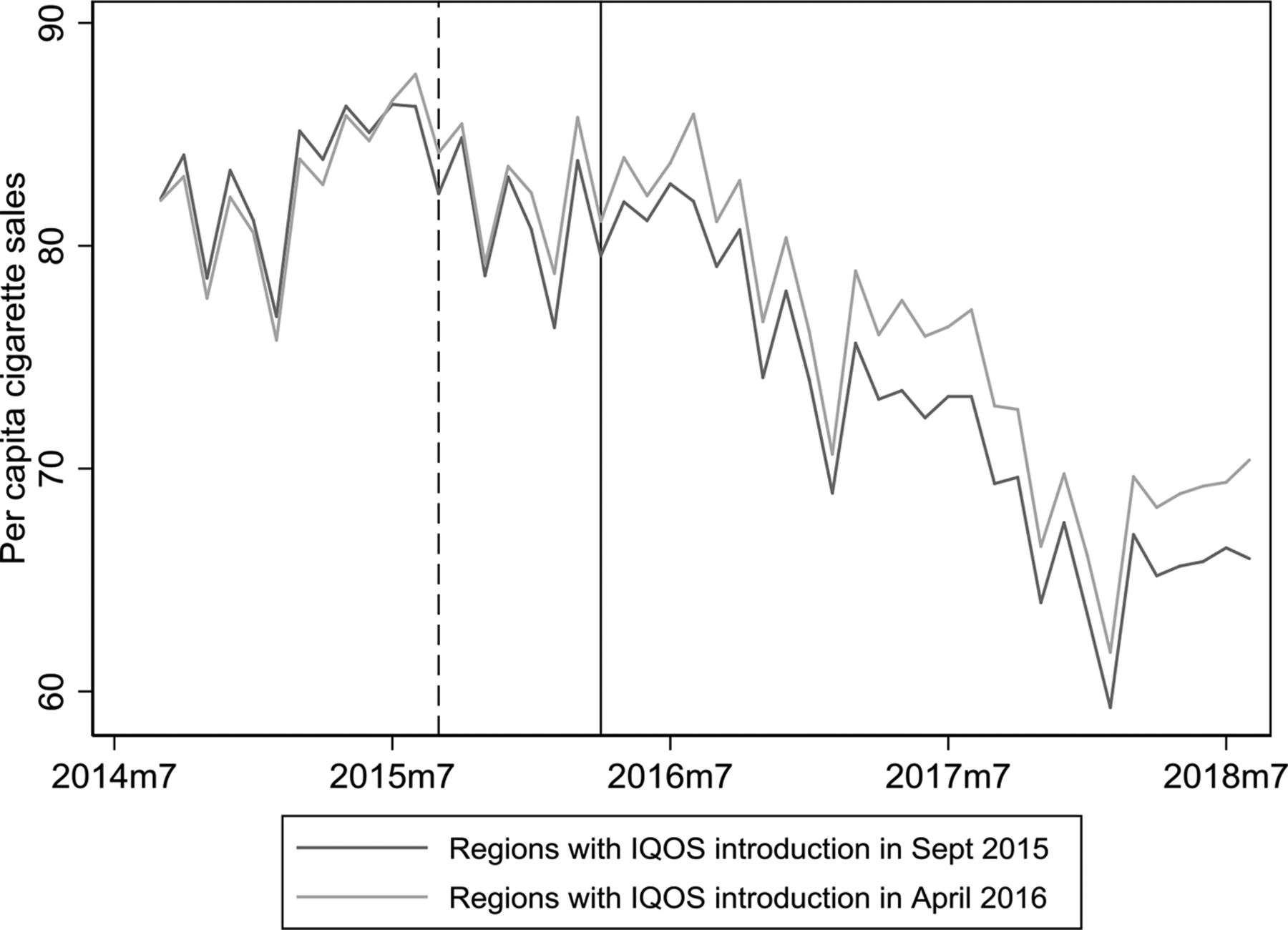
Per capita cigarette sales in regions with earlier versus regions with later IQOS introduction. The dashed vertical line indicates September 2015 IQOS introduction, while the solid vertical line indicates April 2016 IQOS introduction.
The trend lines for per capita cigarette sales were kinked at the time of introduction of IQOS heated tobacco products in each of the 11 Japanese regions. With high values of the Chow test statistics, the null hypothesis of the stability of the trend is rejected (F=254.94, p<0.001 for Approach 1; F=243.27, p<0.001 for Approach 2; F=120.99, p<0.001 for Approach 3). Estimates from the test’s underlying model indicate that, across all regions, per capita cigarette sales were slightly increasing before the introduction of IQOS (at a rate of 0.10 to 0.14 cigarettes per person per month on average, depending on the approach), but started to decline after the IQOS introduction (declining at a rate of 0.63 to 0.66 cigarettes per person per month, depending on the approach). Results from the models using the first, second and third approach to define IQOS regional introduction dates are presented in the online supplementary appendix figures S1, S2 and S3.
Supplemental material
The value of the R2 statistic indicates that the model with region-specific kinks at IQOS introduction fits the trends in cigarette sales in Japan better than any of the placebo models with month-specific kinks that are applied uniformly across all regions. From this result, we can conclude that regional IQOS introduction dates explain the timing of the decline in cigarette sales better than any national-level event, including IQOS national rollout in April 2016.
The model based on the actual dates of introduction ranked in the top 98.5% (5th out of 330) of all possible placebo models with combinations of the original IQOS introduction months redistributed among regions in Approach 1. The model based on the actual dates of IQOS introduction also ranked in the top 92.7% (4th out of 55) possible placebo models in Approach 2, and in the top 86.7% (2nd out of 15) possible models in Approach 3. table 2 presents the goodness of fit of the true introduction date models versus the placebo permutation models in each approach. Online supplementary appendix figures S4, S5,and S6 present the histogram of the R2 statistic for the placebo models in Approach 1, 2 and 3, showing the placement of the test statistic for the introduction date model amidst this null distribution. The results of this randomisation test indicate that it is unlikely that the timing of the observed declines in cigarette sales are unrelated to IQOS introduction.
Goodness of fit of the model with true IQOS introduction months versus placebo models
We performed several additional analyses to check the robustness of the findings presented above. First, the moment of IQOS introduction might not be the best predictor of the onset of declines in cigarettes sales and it might well be the moment of market expansion that would serve better to predict those sales drops. We determined IQOS expansion by establishing an appropriate market volume threshold – the minimum level of sales volume that reliably and consistently predicts immediate and rapid diffusion of IQOS in a given region. However, using market expansion dates instead of market introduction dates in our models did not change the results (see online supplementary appendix). In the second part of the robustness check, we truncated the data by removing observations from April 2016 to August 2018. This created a dataset of a standard natural experiment setting with two groups: the treatment group, which received IQOS in September 2015, and the control group, in which IQOS was not introduced. Using the two-way fixed effects model with the truncated data from Approach 1, 2 and 3, again, did not change the results. The models still indicated that IQOS introduction in September 2015 affected trends in cigarette sales in the treatment group, compared with the control group (p<0.001 in Approach 1, p=0.023 in Approach 2 and p=0.027 in Approach 3).
Discussion
These results show that it is likely that the introduction of IQOS reduced per capita cigarette sales in Japan. It is difficult to come up with alternative explanations that can account for why the month of IQOS introduction predicts when cigarette sales began to decline in each region better than nearly all possible placebo permutations that redistribute IQOS introduction months across regions. Since IQOS introduction, which varied across regions, better predicted the timing of cigarette sales decline than any one time applied to all regions simultaneously, we can conclude that it is relatively less likely that a national-level exogenous shock was the true cause of the observed decline in cigarette sales. In particular, there was no national-level tobacco control legislation implemented around the time of IQOS introduction. Japan adopted its first national smoke-free legislation in mid-2018, but it is being implemented in phases through April 2020.14 The patterns of cigarette use could not be affected by pricing of the products either, since IQOS and cigarette prices did not differ across regions during this period. According to the Intage data, IQOS price remined stable at 21 yen per heat stick across all regions and throughout the analysis. The weighted average cigarette price also remined stable at 20 yen per stick. Attempts to control for monthly household income and seasonality, did not change the models’ results (table 3). Cigarette sales trends might have also been affected by the rollout of products competing with IQOS, British American Tobacco’s Glo and Japan Tobacco’s Ploom Tech, but those products were launched nationally much later than IQOS – in late 2017 and in 2018, respectively15 16 – and their use did not expand nearly as quickly as the use of IQOS.2 Since most existing regulations have been voluntary, industry self-regulations,17 perhaps the implementation of those local regulations coincided with IQOS introduction. Alternatively, PMI could have chosen to introduce IQOS in prefectures that they anticipated would have a rapid decline in sales absent IQOS. However, those scenarios are not likely. In the past, the tobacco industry has been selecting test markets for the new product rollouts to be representative of the total market.18–20 Therefore, a far more likely scenario in Japan is that PMI chose places for the early-stage IQOS introduction to be representative of a national rollout. This created a natural experiment, which we utilised.
Goodness of fit of the model with true IQOS introduction months versus placebo models (controlling for household income and seasonality)
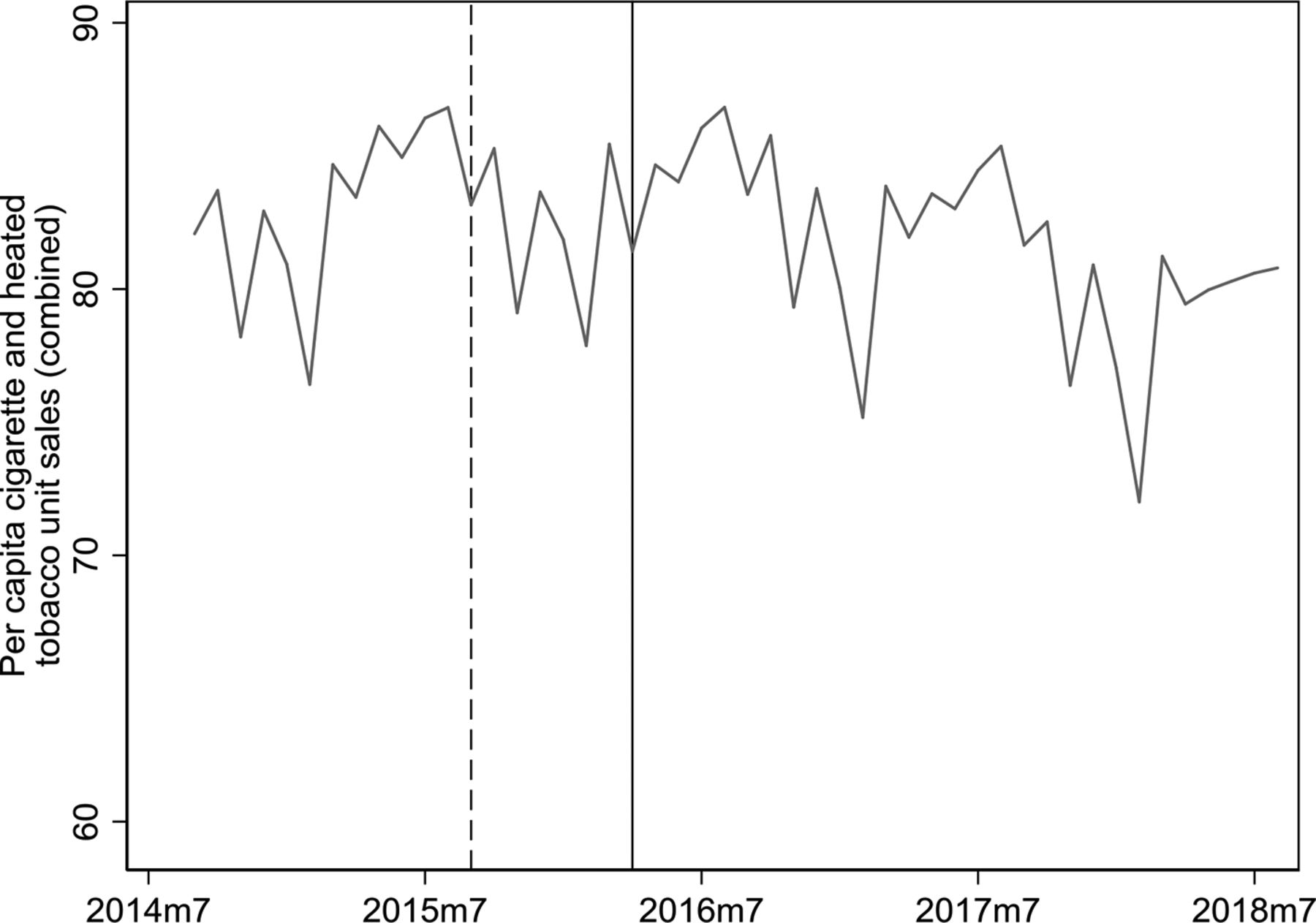
The population health impact of replacement of IQOS sales for tobacco cigarette sales in Japan is highly dependent on factors that cannot be determined from sales data alone. Every cigarette consumed has a causal impact on disease, but a sales reduction driven by reduced smoking initiation or increased smoking cessation would have far more clinical meaning than one driven by prolonged reduction in smoking intensity among dual users (eg, using both cigarettes and IQOS). Also, when using PMI’s product equivalence rate of one heat stick per cigarette,21 it appears that the combined sales of IQOS and tobacco cigarettes are relatively stable in Japan during this period (figure 2). However, it is unknown whether the availability of HTPs will lead to more or to less total tobacco product use over time. Perhaps most importantly, unless smokers are using IQOS as a short-term cessation device, the causal mechanism by which smoking is reduced entails assuming the highly uncertain and potentially substantial risks associated with prolonged use of IQOS.

{kind=link}
{kind=link}
Combined per capita cigarette and IQOS heat stick sales in Japan.The dashed vertical line indicates September 2015 IQOS introduction, while the solid vertical line indicates April 2016 IQOS introduction.
Presently, we cannot make confident conclusions about the level of direct harm to users and how this compares to the harms of smoking. There are no long-term studies that compare disease rates of IQOS users to either smokers or non-smokers who do not use IQOS, nor is there an established process of inferring disease risk from the information that is available, including measures of exposure to certain chemicals or assessments of short-term health indicators and biomarkers. Indeed, the lowered exposure in the context of lower intensity smoking has shown that relative risk can be highly disproportionate to relative exposure.22 23 Studies that examine exposures of known toxins in IQOS aerosol have generally found substantially lower levels than conventional cigarette smoke.24 25 However, IQOS delivers higher levels of many other chemicals of unknown toxicity,26 and IQOS exposures to known toxins are significantly higher than those of non-tobacco vapour products, such as e-cigarettes.27 28 Similarly, the cytotoxicity of IQOS emissions on bronchial epithelial cells was found to be significantly lower than a Marlboro cigarette, but significantly higher than a MarkTen non-tobacco vapour product.29 Human biomarker studies mostly come from industry sources at this time, which have obvious potential conflicts of interest; nevertheless, most of these studies demonstrate that reductions of exposure in aerosol appear to translate to reductions in urine metabolites.30 31 Given that IQOS relative risk profile is not yet agreed on, replacing cigarette sales with IQOS is going to have an indeterminate effect on health.
Patterns of IQOS use and smoking in Japan may not generalise to other countries or products. Higher rates of adoption of charcoal filter cigarettes in previous decades may be evidence of a greater priority being placed on perceived reductions in harm among Japanese smokers.32 Unique characteristics of the Japanese regulatory environment may also play a role, including a highly-restrictive approach to non-tobacco vapour products such as e-cigarettes,33 34 perhaps increasing the likelihood that HTPs substitute for higher-exposure tobacco cigarettes as opposed to lower-exposure electronic nicotine delivery systems, such as e-cigarettes.
There are several limitations to the methodological approach. First, the use of more standard economical methods of establishing product substitutability, such as using seemingly unrelated regressions to estimate cross-price elasticities of product demand, was not possible due to little variation in the price variable. Prices of IQOS and cigarettes were comparable between the products and stable across regions throughout the analysis making the standard demand analysis inexecutable. Second, our measure of product use is not perfect. Sales might not exactly reflect product use, with some of the purchased product being never used or used in the later periods, and some of the product purchased in one region and being used in another region. Third, our data capture cigarette sales in Intage-participating stores only. However, cigarette sales captured by Intage (109 billion sticks sold in 2017) account for 72% of the total cigarette market in Japan from Euromonitor International (151 billion cigarettes sold in 2017),35 suggesting the Intage market coverage data are considerable but not complete. Similarly, the trends in cigarette sales from Intage are consistent with those from Euromonitor. Just like the Intage data, Euromonitor data indicate that cigarette sales were relatively stable before IQOS introduction in Japan (1.8% average annual decline from 2011 to 2015), but significantly declined during and after IQOS introduction (9.5% average annual decline from 2015 to 2018).35 Lastly, specific aspects of the Intage’s methods used to estimate regional market sizes based on data from a sample of stores, the details of which are not available to us, might affect our results. Nevertheless, despite these challenges, the models produce results that are significant and robust.
Conclusion
The example of IQOS in Japan demonstrates a circumstance in which cigarette consumption has likely been reduced via the introduction of an alternative non-combustible tobacco product. Definitively identifying that the introduction of a novel tobacco product is significantly changing the marketplace for tobacco products is important information for policymakers and public health proponents as they consider how to alter existing tobacco control policies to accommodate these new products. The mechanisms that drove these changes in Japan deserve more attention from scholars to identify what lessons in policy formation ought to be transferred to other jurisdictions. The net population health impact, however, cannot be assessed without resolving several uncertainties related to the direct harms of HTPs and patterns of both smoking and HTP use.
What this paper adds
The tobacco users' switching between different product types might not be purely driven by price differences across products, but rather by growth in variety of products that are available on the market, some of which may be less harmful or more appealing than traditional combustible tobacco products.
The study utilizes a natural experiment created during the rollout of a novel heated tobacco product, IQOS, in 2015 and 2016 in Japan and shows that the introduction of IQOS in a region predicts a decline in per capita cigarette sales in that region.
Cigarette sales have likely been reduced through the rollout of IQOS, while combined product volumes remained unchanged.
The net public health effect is uncertain and will depend on the specific patterns of smoking behaviour driving this decline as well as the direct harm of IQOS to users.
Acknowledgments
We would like to thank Dr. Takahiro Tabuchi who provided useful insights into IQOS introduction in Japan, as well as Qing Li and Aidan Larsen for their help with data gathering from the Japan Statistical Office.
References
Footnotes
Contributors MS and ZC designed the study. MS conducted the analysis. MS and ZC wrote the first draft of the manuscript. All authors contributed to interpretation of results and to refinement, writing and editing of the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The contents of this article are the sole responsibility of the authors and do not necessarily represent the positions of the American Cancer Society.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement For proprietary reasons, the data used in this manuscript cannot be
made available to all potential users.