Article Text

Abstract
Background Secondhand tobacco smoke (SHS) exposure is a global public health problem. Ghana currently has no legislation to prevent smoking in public places. To provide data on SHS levels in hospitality venues in Ghana the authors measured (1) airborne particulate matter <2.5 μm (PM2.5) and nicotine concentrations and (2) hair nicotine concentrations in non-smoking employees. Quantifying SHS exposure will provide evidence needed to develop tobacco control legislation.
Method PM2.5 was measured for 30 min in 75 smoking and 13 non-smoking venues. Air nicotine concentrations were measured for 7 days in 8 smoking and 2 non-smoking venues. Additionally, 63 non-smoking employees provided hair samples for nicotine analysis.
Result Compared to non-smoking venues, smoking venues had markedly elevated PM2.5 (median 553 [IQR 259–1038] vs 16.0 [14.0–17.0] μg/m3) and air nicotine (1.83 [0.91–4.25] vs 0.03 [0.02–0.04] μg/m3) concentrations. Hair nicotine concentrations were also higher in non-smoking employees working in smoking venues (median 2.49 [0.46–6.84] ng/mg) compared to those working in non-smoking venues (median 0.16 [0.08–0.79] ng/mg). Hair nicotine concentrations correlated with self-reported hours of SHS exposure (r=0.35), indoor air PM2.5 concentrations (r=0.47) and air nicotine concentrations (r=0.63).
Conclusion SHS levels were unacceptably high in public places in Ghana where smoking is allowed, despite a relatively low-smoking prevalence in the country. This is one of the first studies to ascertain SHS and hair nicotine in Africa. Levels were comparable to those measured in American, Asian and European countries without or before smoking bans. Implementing a comprehensive smoke-free legislation that protects workers and customers from exposure to secondhand smoke is urgently needed in Ghana.
- Environmental tobacco smoke
- public policy
- surveillance and monitoring
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Background
Exposure to secondhand tobacco smoke (SHS) is a global public health problem as recognised by environmental, occupational and public health authorities.1–4 Of all public places, restaurants and bars have the highest SHS concentrations,5–8 increasing the cardiovascular, respiratory and cancer risks among non-smoking workers and patrons.1 9 10 To protect all people from the health effects of SHS, the Framework Convention on Tobacco Control (FCTC) legally binds signatory countries to implement legislations that eliminate smoking in all indoor public places and workplaces.2 11 Political influence of multinational tobacco companies remains a major obstacle for the implementation of smoke-free legislations in African countries.12 Indeed, despite the large number of African countries that have ratified the FCTC (39 as of July 2009), only a few (Djibouti, Kenya, Mauritius, Niger and South Africa) have passed legislation addressing tobacco control in public places.12 13
Ghana ratified the FCTC in November 2004. While a draft tobacco control bill was presented in 2005, the bill has not yet been passed into law.14 Moreover, data on SHS levels in public places and workplaces remain largely unknown in Ghana and in Africa, in general. Concentrations of airborne particulate matter <2.5 μm (PM2.5) and nicotine have been used to assess SHS exposure in public places in the Americas, Asia and Europe.5–8 15 16 Biomarker concentrations among non-smokers are useful to quantify overall personal exposure,17 with hair nicotine concentrations being widely used as a non-invasive biomarker for long-term SHS exposure.18–21
In this study, our goal was to provide objective data on indoor SHS exposure in restaurants, bars and other hospitality venues in Ghana by measuring airborne PM2.5 and nicotine concentrations. In addition, to quantify SHS exposure among hospitality employees, hair nicotine concentrations were measured in non-smoking employees. This study can guide public health and policy interventions to protect the population of Ghana from the health consequences of exposure to tobacco smoke, as mandated by the FCTC.
Methods
Study population
This cross-sectional assessment was conducted in Accra (the capital city) and other towns across Ghana (Akosombo, Kintampo, Kumasi, Nkawkaw, Takoradi, Tamale and Tema) between June and August 2007. The towns were selected on a convenience basis and represented different geographical and economical sectors within the country. PM2.5 concentrations were measured in 88 restaurants/bars/nightclubs/casinos located in the popular entertainment districts within each city (from 1 in Akosombo and Kintampo to 60 in Accra depending on the size of the city). The venues were recruited using a door to door technique (in small cities only one venue was recruited as the field workers travelled from one city to another). In Accra and Tema (a major town near Accra), a subset were invited to participate in a further assessment of air nicotine concentrations. For airborne nicotine, the owner had to agree and ≥3 non-smoking employees had to be willing to provide a hair sample and answer a questionnaire. Among the 12 venues invited, 10 agreed to participate (response rate 83%). The study was approved by the Ghana Health Service Ethical Review Committee and Institutional Review Boards at the Johns Hopkins Bloomberg School of Public Health and Yale University.
Data collection
Real-time PM2.5 concentrations were measured for ≥30 min (median 46 min) using TSI SidePak AM510 Personal Aerosol Monitor (TSI Inc., Shoreview, Minnesota, USA) with a 0.32 calibration factor22 and following an established protocol.8 The number of actively burning cigarettes (recorded every 15 min) and room dimensions (measured using a sonic measuring device) were used to calculate active smoking density (average number of burning cigarettes per 100 m3). Information on other burning sources was collected.
Vapour-phase nicotine was estimated for 7 days using passive samplers (two per venue).15 23 Samplers were shipped to the Johns Hopkins Bloomberg School of Public Health for the analysis of nicotine concentrations (μg/m3) using gas chromatography with nitrogen-selective detection. The detection limit (DL) was 0.003 μg/m3. One sample <DL was replaced by DL/2.
Hair samples from non-smoking employees (n=69) were collected on the day the nicotine samplers were installed. A small hair sample (∼30–50 strands) was cut near the root from the back of the scalp and placed in a labelled sealed plastic bag. Up to 3 cm of hair from the scalp was used to evaluate SHS exposure during the most recent months. After sample preparation, nicotine was analysed using an established protocol.24 The limit of detection was 0.02 ng/mg for a 30 mg hair sample.
Questionnaire
The 10 managers/owners and 69 non-smoking employees who participated in the air nicotine and hair nicotine assessment were interviewed by trained field workers. The managers/owners were asked to describe general characteristics of the venue (table 1). The employees were asked about sociodemographic information, smoking history and SHS exposure in different environments and opinions on smoke-free legislation. The interviews were voluntary and each participant signed informed consent.
Characteristics of the hospitality venues by smoking status
Statistical analysis
Average PM2.5, air nicotine and hair nicotine concentrations were described using the median, IQR and range stratifying by the smoking policy of the venue. Scatter plots and Spearman's correlation coefficients were used to evaluate the relationship between PM2.5 and air nicotine concentrations and between hair nicotine with the following SHS measures: self-reported hours of exposure, PM2.5 concentrations and air nicotine concentrations. Statistical analysis was performed using SAS 9.1 statistical software.
Results
Indoor air PM2.5 concentrations
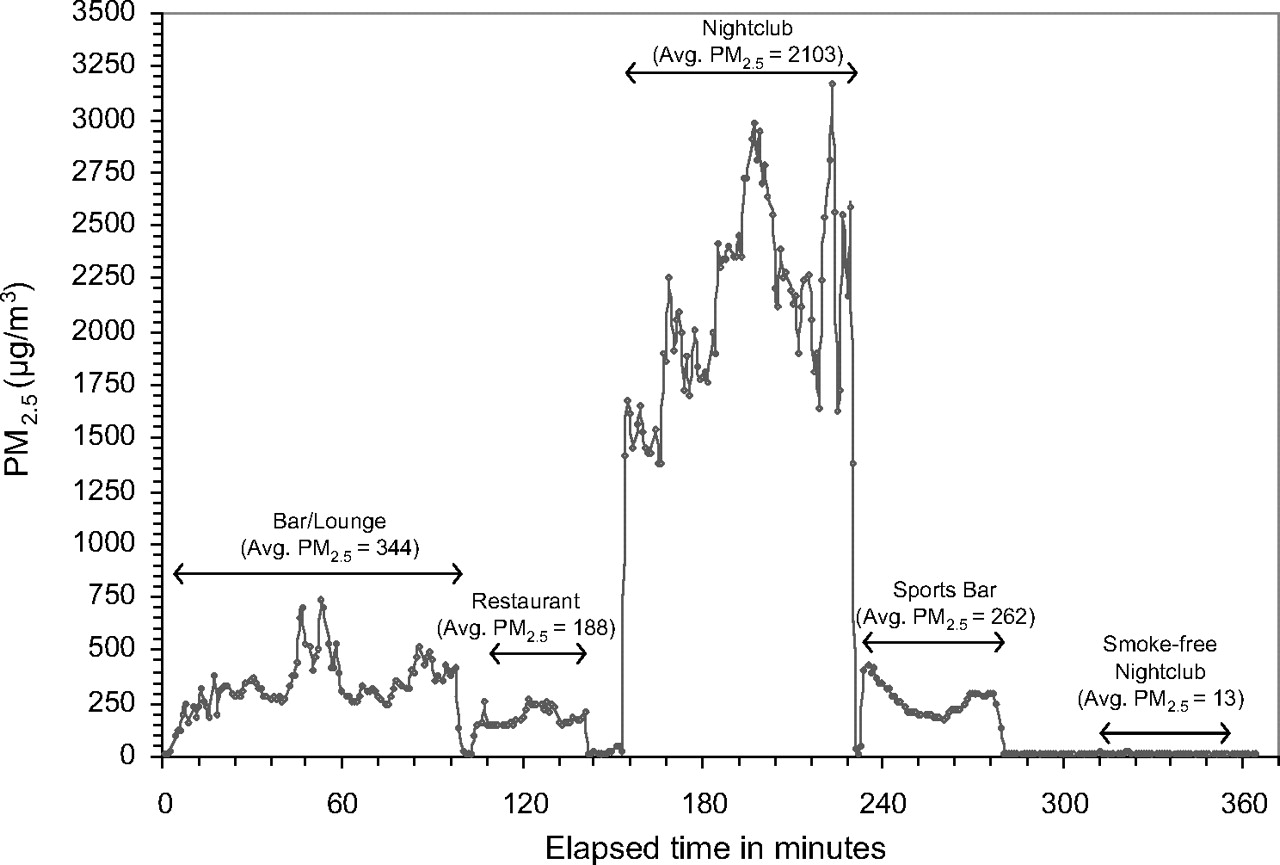
Median (IQR, range) average PM2.5 concentrations in 75 smoking venues (smoking observed during the sampling period) were 553 (259–1038, 3–2103) μg/m3 compared to 16 (14–17, 12–30) μg/m3 in 13 non-smoking venues (smoking not observed during the sampling period). Real-time PM2.5 concentrations for the first five venues are shown in figure 1. No other visible PM2.5 source was observed. Smoking venues in Accra had higher average PM2.5 concentrations (median 688 μg/m3) compared to other cities (596 μg/m3). In smoking locations, mean (SD) active smoking density was 8.0 (5.0) burning cigarettes per 100 m3. Average PM2.5 concentrations were positively correlated (Spearman's correlation coefficient 0.55, p<0.001) with active smoking density.

Real-time PM2.5 concentrations in the first five venues.
Air nicotine concentrations
Air nicotine concentrations were measured in eight smoking venues (no smoking restriction) and two smoke-free venues (voluntary policy as reported by the owner/manager) (table 1). Median (IQR, range) air nicotine concentrations were 1.83 (0.91–4.25, 0.33–6.01) μg/m3 in smoking venues compared to 0.03 (0.02–0.04, <0.003–0.04) μg/m3 in smoke-free venues (p=0.012). Nicotine concentrations were borderline significantly higher in venues with dancing space (4.27 vs 1.52 μg/m3, p=0.07). Other characteristics (occupancy, number of employees, food, music or outdoor space) were not related to air nicotine concentrations. PM2.5 concentrations comparing the eight smoking venues (median 905 μg/m3) to the two smoke-free venues (median 26.5 μg/m3) were also markedly different (p<0.001). Air nicotine concentrations were strongly and positively correlated with PM2.5 concentrations, r=0.76, p<0.001. A 10-fold increase in air nicotine concentrations was associated with a 4.6-fold increase in PM2.5 concentrations (95% CI 2.0–10.1).
Hair nicotine concentrations
Non-smoking employees working in smoking and non-smoking venues were of similar age, gender, education status, employment duration and shift length (data not shown). About 8% of employees were former smokers and 7% lived with a smoker; 76% supported comprehensive smoke-free laws.
Hair nicotine concentrations were markedly increased in non-smoking employees working in smoking venues (median 2.49, IQR 0.46–6.84, range 0.07–48.4 ng/mg) compared to non-smoking employees working in smoke-free venues (0.16, 0.08–0.79, undetectable-0.79 ng/mg). Hair nicotine concentrations were positively correlated with self-reported hours of SHS exposure (r=0.35), PM2.5 concentrations (r=0.47) and air nicotine concentrations (r=0.63) (figure 2). The results were similar after excluding participants who lived with a smoker.

{kind=link}
{kind=link}
Scatter plots of the relationship of hair nicotine concentrations (ng/mg) with different measures of secondhand smoke exposure in the workplace (hours of exposure per week, air PM2.5 concentrations and air nicotine concentrations). Dots correspond to hair nicotine concentrations for each non-smoking employee by employee self-reported hours of exposure (top panel), log-transformed PM2.5 concentrations (left bottom panel) and log-transformed air nicotine concentrations (right bottom panel) in each venue. The line estimates the corresponding log-linear dose–response relationships.
Discussion
In this study, we found high levels of SHS exposure in bars and restaurants in Ghana. Airborne PM2.5 concentrations measured over >30 min at a time of normal occupancy were approximately 35 times higher in smoking compared to non-smoking venues and strikingly higher than 25 μg/m3, the 24-h WHO outdoor air quality standard that has been adopted by Ghana as a guideline for the protection of public health.25 Air nicotine concentrations measured over a week were approximately 60 times higher in smoking versus smoke-free venues. Finally, hair nicotine concentrations were approximately 16 times higher in non-smoking employees working in smoking venues compared to non-smoking employees working in smoke-free venues.
SHS levels measured in this study were similar and sometimes higher than airborne PM2.5 and nicotine concentrations measured in American, Asian and European countries without or before implementing comprehensive smoke-free legislations.5–8 16 26–30 Mean active smoking density in venues was also among the highest compared to studies conducted in other countries.27–30 While smoking prevalence in Ghana is relatively low,31 these results provide objective evidence that SHS exposure is a major indoor pollutant in bars and restaurants in Ghana, posing serious health risks for patrons and employees spending time in those environments.
Ghana is currently in the process of regulating smoking in public places and workplaces. There are renewed efforts to get the draft bill presented to the cabinet and several civil society organisations are urging the government to expedite the passage of the tobacco control bill into law. However, similar to other countries in Africa, implementing smoke-free legislation remains a challenge.12 14 The high levels of SHS exposure measured in this study, the fact that there is no safe level of SHS,1 10 and recent experiences showing that incomplete smoking bans are more difficult to implement32 33 compared to comprehensive ones,34–36 reinforce the urgent need to enact a comprehensive smoke-free legislation that protects all people, including workers, from SHS exposure in Ghana.
Previous studies assessing SHS concentrations in indoor environments have generally measured PM2.5 or nicotine. In our study we measured both, confirming a strong positive relationship between PM2.5 concentrations measured over >30 min and air nicotine concentrations measured over 7 days, consistent with previous US studies in homes and office buildings.37–39 Because nicotine is tobacco specific, these results confirm that tobacco smoke was the most likely source of particulate matter and that randomly measuring PM2.5 over a short period reflects SHS in most indoor environments. Our study also compared diverse markers of SHS (PM2.5, nicotine and self-reported hours of exposure) with hair nicotine, a biomarker of internal dose. Hair nicotine concentrations were moderately correlated with self-reported hours of exposure and with 30-min average PM2.5 concentrations. The strong correlation between air and hair nicotine is consistent with the strong correlation between air nicotine and serum cotinine in chamber experiments.40
To our knowledge this is the first study measuring hair nicotine concentrations in a population of non-smoking employees in a Sub-Saharan African country. Our results are consistent with hair nicotine concentrations measured in bar and restaurant workers before a total ban in New Zealand.18 SHS exposure among hospitality employees is of concern given the long hours of exposure and high density of smokers in these environments. Before the implementation of smoke-free legislations in the USA, SHS exposure in non-smoking bar and restaurant employees was between 1.5 and 4.4 times higher compared to non-smokers who lived with smokers.41
Study employees highly supported comprehensive smoke-free legislations, consistent with other countries.42 43 Conversely, most owners/managers indicated it was very unlikely for their establishments to go voluntarily smoke free. Among those who responded, 50% claimed customer preference and concerns over profit loss as the reasons for allowing smoking. Studies in other countries, however, have found no decline or even improvement in bar/restaurant business after the implementation of comprehensive smoke-free legislations.44 45
The study was limited by a small sample size and a non-random sampling strategy. However, several cities/towns were sampled. In Accra, moreover, several neighbourhoods were included. We could thus characterise exposure in venues that are meaningful to many people and workers in Ghana. Air nicotine measured over 7 days most likely underestimated exposure during actual working hours. For hair nicotine, chemical treatments may have reduced nicotine concentrations.21 However, the correlation between air and hair nicotine was strong suggesting that both measures provided consistent exposure estimates. Study strengths include the use of established SHS methods, the large number of places with PM2.5 measurements and the high response rate for air and hair nicotine assessment. Having PM2.5 and air nicotine concentrations was an important strength as we clearly showed that SHS was the most important contributor to PM2.5 in Ghana.
In conclusion, SHS exposure was markedly elevated in public places and workplaces where smoking is allowed in Ghana. This is the first study to describe levels of PM2.5 and air nicotine concentrations in hospitality venues and hair nicotine concentrations in non-smoking employees in Ghana. The levels were high, similar to those found in American, Asian and European countries without smoke-free legislation. The finding of unacceptably high levels of SHS in hospitality venues and high levels of hair nicotine in non-smoking employees working in these venues provide a strong basis for implementing a comprehensive smoke-free legislation in Ghana.
What this paper adds
In Ghana, as in most countries in Africa, little is known about the extent of secondhand smoke (SHS) exposure in public places. This study measured particulate matter of 2.5 μm (PM2.5) and air nicotine concentrations in hospitality venues and hair nicotine concentrations in non-smoking employees in Ghana.
SHS levels were unacceptably high in public places in Ghana where smoking is allowed, comparable to those measured in American, Asian and European countries without or before smoking bans.
Implementing a comprehensive smoke-free legislation that protects workers and customers from SHS exposure in indoor public places is urgently needed in Ghana.
Acknowledgments
The authors thank the staff of the Research and Development Division, Ghana Health Service (GHS) and Professor Badu Akosa (Fmr. Director General of GHS) for their collaboration, the Ghana Tourist Board for their support with conducting the fieldwork, Cheryl Higbee (Department of Health Behavior, Roswell Park Cancer Institute) for support in particle analyses and Chrissy Torrey and Jie Yuan (Exposure Assessment Laboratory, Johns Hopkins Bloomberg School of Public Health) for support with conducting air and hair nicotine analyses.
References
Footnotes
Funding Funding for this project was provided by the Flight Attendant Medical Research Institute (FAMRI); IDRC-Research for International Tobacco Control, Canada; Bloomberg Global Initiative, Johns Hopkins Bloomberg School of Public Health; and the Stolwijck Fellowship, Yale University. The authors, and not the funding sources, are responsible for the design and conduct of the study, the collection, the analysis and interpretation of the data and the preparation of the manuscript.
Competing interests None.
Ethics approval The study and consent procedures were approved by Ghana Health Service Ethical Review Committee and by Institutional Review Boards at Johns Hopkins Bloomberg School of Public Health and Yale University. Participation of subjects was voluntary and after receiving informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.