Article Text

Abstract
Objectives Female smoking is predicted to double between 2005 and 2025. There have been numerous calls for action on women's tobacco use over the past two decades. In the present work, evidence about female tobacco use, progress, challenges and ways forward for developing gendered tobacco control is reviewed.
Methods Literature on girls, women and tobacco was reviewed to identify trends and determinants of tobacco use and exposure, the application of gender analysis, tobacco marketing, the impact of tobacco control on girls and women and ways to address these issues particularly in low-income and middle-income countries.
Results Global female tobacco use is increasingly complex, involving diverse products and factors including tobacco marketing, globalisation and changes in women's status. In high-income countries female smoking is declining but is increasingly concentrated among disadvantaged women. In low-income and middle-income countries the pattern is more complex; in several regions the gap between girls' and boys' smoking is narrow. Gendered analyses and approaches to tobacco control are uncommon, especially in low-income and middle-income countries.
Conclusions Tobacco control has remained largely gender blind, with little recognition of the importance of understanding the context and challenges of girl's and women's smoking and secondhand smoke exposure. There has been little integration of gender considerations in research, policy and programmes. The present work makes a case for gender and diversity analyses in tobacco control to reflect and identify intersecting factors affecting women's tobacco use. This will help animate the WHO Framework Convention on Tobacco Control's concern for gender specificity and women's leadership, and reduce the impact of tobacco on women.
- Advertising and promotion
- qualitative study
- young adults
- cessation
Statistics from Altmetric.com
Introduction
Tobacco use, particularly cigarette smoking, has long been recognised as an important threat to girl's and women's health in high-income countries (HICs) and is increasingly recognised as an important threat to girls' and women's health in low-income and middle-income countries (LMICs) where the epidemic is growing. This health threat has three main facets: tobacco use by women, exposure to secondhand smoke (SHS) from male smokers and the diversion of family resources from food, shelter, healthcare and education to purchase tobacco products.
The past 20 years have seen numerous calls for action on women and tobacco, and for considering the impact of tobacco on maternal and child health and on women's economic well-being.1–11 However, tobacco control in HICs and LMICs has remained largely gender blind. There has been little recognition of the importance of understanding the context and challenges of girls' and women's smoking and exposure to SHS, and the increase in women's smoking in LMICs.1 6 12 Thus, many opportunities for knowledge generation and effective responses to women's tobacco use remain lost or overlooked.
While the omission of gender affects our understanding and response to women's and men's tobacco use, this paper focuses on girls and women. We also focus largely on cigarette smoking as accurate data on women's smokeless tobacco use are available for only a minority of countries. In this paper we describe what is known about patterns, trends and determinants of girl's and women's tobacco use and SHS exposure, the importance of gender analysis, the marketing of tobacco to girls and women, the impact of tobacco control and potential future directions in addressing these issues, particularly in LMICs.
Girls' and women's tobacco use
The global prevalence of smoking is currently far higher among men than women, 41.1% versus 8.9% in 200513 (table 1). However, global male smoking rates have peaked and are on the decline while women's rates are still rising.14 Furthermore, the gap between men's and women's smoking prevalence is small in the regions of the Americas and Europe, and in high-income and upper-middle-income countries. In contrast, in the majority of low-income and low-middle-income countries (and in the regions of Africa, Southeast Asia, Eastern Mediterranean and Western Pacific) women's smoking prevalence remains under 5%. However, regional and individual country estimates often mask vast disparities in women's prevalence between and within countries, due to such factors as socioeconomic status (SES), educational attainment, race/ethnicity and geography. Prevalence data show that despite important regional differences, the gap between boys' and girls' cigarette smoking is far narrower than that between adult men and women in all regions (table 2).15 16 Accurate data on tobacco use during pregnancy and women's SHS exposure are available for only a minority of countries.12 17
Prevalence of smoking any tobacco product, adults ≥15 years, 2006
Cigarette smoking and other tobacco product use, girls and boys, aged 13–15 years, 1999–2008
Current global trends indicate that smoking by women is on the rise and is increasingly associated with disadvantage, whether measured by education, income or other indicators of social exclusion.18–20 In countries with the longest history of women's smoking such as the USA, Canada, Australia and in Western Europe, smoking is already concentrated in the most disadvantaged groups. In several European countries, including the UK, Norway and Spain, the highest smoking uptake rates are now seen in disadvantaged girls.22
A recent analysis of World Health Survey data from 50 countries19 shows how tobacco use is spreading from HICs to LMICs, particularly among disadvantaged groups, and how these trajectories differ by gender, age and stage of diffusion of smoking in a country (as described in the four-stage cigarette smoking epidemic model of Lopez and colleagues23). This analysis reveals that the key drivers of the tobacco epidemic such as increasing gross domestic product in LMICs (which increases cigarette purchasing power) and increasing educational status (which increases awareness of health risks) have a differential impact on women and men, and are mediated by gendered social, cultural and economic factors. These factors include social norms and restrictions on women's smoking, as well as shifts in women's social and economic status.
Women's emancipation and increases in status have long been associated with increases in smoking. Young urbanised women are often among the first to adopt cigarette smoking in LMICs. The link between gender empowerment (measured by economic and political participation) and smoking has been positively correlated,24 establishing that as the gender empowerment measure for women rises, so does the gender smoking ratio. While the correlation of women's status with smoking uptake may explain initiation, it may not explain the economic and gendered patterns of smoking once diffusion has occurred.25 For example, Pampel,26 using a complex set of indicators to measure a ‘gender-equality’ hypothesis that included social and cultural as well as economic independence, concluded that there was no support for a causal relationship between increased equality and increased smoking among women in HICs. Strategies aimed at addressing the smoking epidemic in women therefore need to be grounded in a multifaceted understanding of women's smoking patterns and trends, and how gender intersects with social position, identity, ethnicity and religion.27
The health impact of women's tobacco use and exposure to SHS
Although women and men who smoke share excess risks for many diseases, women also experience risks that are unique to them or that are higher in women compared to men.4 28 29 Smoking is causally linked to cervical cancer, a leading cause of death from cancer among women in LMICs.30 Some evidence links active smoking and exposure to SHS to increased risk of breast cancer.31 A recent systematic review and meta-analysis found that, compared with non-smokers, women smokers have a 25% greater RR of coronary heart disease than male smokers, after controlling for other cardiovascular risk factors.32 The negative health impact of maternal smoking on fetal development has been well documented.33
Limitations in research on girls, women and tobacco
While there has been an upsurge in research on gender and tobacco over the past two decades, including studies on the health effects of smoking and the determinants of smoking uptake and cessation,28 29 this has been limited in several important respects.
Defining gender
To date, studies have been limited in their treatment and understanding of sex and gender. Biological and physiological factors (‘sex’) and social, economic and cultural influences (‘gender’) have, when considered at all, been conceptualised and treated as distinct and separate domains. However, recent theoretical arguments have shown that sex and gender are often inseparable concepts and that their effects are interactive and blended.35 Sex and gender also each exist on continua, making the notion of ‘differences’ less relevant than developing more nuanced measures of sex/gender factors, particularly in research design.36 37 These advances pose theoretical and methodological challenges for gender and diversity analysis in tobacco control. Potential strategies for addressing these challenges include the use of relevant training manuals and texts,36–40 requiring or providing guidelines for consideration of sex, gender and related factors for research funding, as is done by the Canadian Institutes for Health Research and US National Institutes of Health,41 42 or for publication in tobacco control journals. Similar approaches are relevant to practice and programme design—particularly those that engage gender and diversity considerations in assessing better practices or developing clinical or public health guidelines (eg, the WHO report Gender Analysis in Health: A Review of Selected Tools 43).
Gender and diversity
In addition, relatively few studies of women smokers have explored the ways in which gender intersects with other dimensions of diversity including age, disadvantage, religion, SES, occupation and race/ethnicity to create conditions and complexities that increase the risk of tobacco use and/or SHS exposure.44 45 Some research in HICs has used quantitative and qualitative methods to undertake nuanced and sophisticated analyses which explore tobacco use and exposure in the context of the diversity of girls' and women's lives, circumstances and experiences.44 46–48 These approaches have shown how women's risks of becoming and remaining smokers relate to gendered and disadvantaged life trajectories and biographies that often include early pregnancy, lone motherhood, deprivation and violence.44 49 In addition, women with the least success in quitting often live in environments where smoking is normative and there is little support for quitting.47
Smoking initiation studies have found that the meanings that young people attach to smoking are gendered and smoking may act as a marker of gender and identity.50–52 Gender differences have been found in HICs with regard to the perceived value of smoking in relation to, among other factors, affect control, creating and maintaining social relationships, body image, weight control, enhancing social identity and status (social capital), and as self-medication.44 46–48 53 54 Some studies have also found that women have greater difficulty quitting compared to men.55 Although the mechanisms are not well understood, they are probably related to biological and psychosocial aspects of addiction and dependence.56 57 Several studies have found that nicotine replacement therapy is less effective in women than men.58–60 Non-nicotine cues to smoke appear to be more important for women than for men, and smoking has a perceived functional value in the lives of low-income single mothers, who use smoking to cope and provide care in disadvantaged circumstances, making cessation more difficult.48 61
A narrow focus on HICs
Most studies have been carried out in HICs where the patterns and trajectories of girls' and women's tobacco use and SHS exposure differ from those in LMICs. Few studies have explored the interaction between gender and smoking uptake and/or cessation in LMICs. While studies conducted in the Philippines and Indonesia found similar reasons for female smoking uptake and continuation as in HICs,62 63 few studies have explored protective factors within specific cultural contexts that promote resiliency in women and girls and serve to inhibit smoking.64 Studies in HICs have shown how unequal power relationships and restricted living circumstances can limit women's ability to reduce exposure to SHS for themselves and their children, arising from smoking by others (usually men) in the home and workplace.65–70 In LMICs, where women's social, political and economic power is often limited, women have even less ability to protect themselves and their children from exposure to SHS from male smokers.71 72
Marketing of tobacco to girls and women
The limited response of the tobacco control community in applying gender and diversity based analyses to tobacco control contrasts starkly with the comprehensive gendered approach of the tobacco industry. Given their low smoking prevalence, women and girls in many countries represent a vast ‘untapped market,’ and a prime target of the tobacco industry. The tobacco industry appears increasingly focused on LMICs, where it has long been culturally inappropriate for women and girls to smoke. In developing its marketing campaigns, the tobacco industry builds on over 80 years of experience of successful gender sensitive and specific marketing to women in HICs.73 In the early 20th century, cigarette companies in HICs learnt that ‘cultural mores may be shifted by design’ to ‘engineer’ the consent of women smokers.74 Numerous studies have shown that global advertising to women seeks to link smoking to desirable female attributes such as independence, modernity, glamour, stress relief and weight control.28 73 75 76
Increasingly in LMICs, upscale young women feature in cigarette advertisements. In Indonesia, recent advertisements for a popular young adult brand feature an affluent, attractive, modern woman using a cell phone. The caption, ‘Yesterday is gone, Clas Mild is Today’, implies that smoking is a behaviour to which a modern woman should aspire (figure 1).76 Depicting women in tobacco advertising in cultures where women do not smoke helps to normalise the association between women and tobacco.62

Clas Mild advertisements from Indonesia.
Brands also employ particular features such as cigarette size, ‘taste,’ images and packaging to attract women. In recent years in HICs, brands including Vogue, Silk Cut and Virginia Slims have introduced ‘purse packs’—small lipstick sized boxes containing ‘Superslim Light’ cigarettes which are half the size of regular cigarettes (figure 2).75 76 Slim cigarettes in feminised packs are increasing in LMICs.75 77 In Indonesia in 2009, the first superslim clove cigarette was introduced for women (A-Volution), which is packaged in a lipstick tube shape.78 More than 100 brands of slim and super slim cigarettes are available in the Russian Federation, some featuring packs designed by fashion designers (figures 3 and 4).79
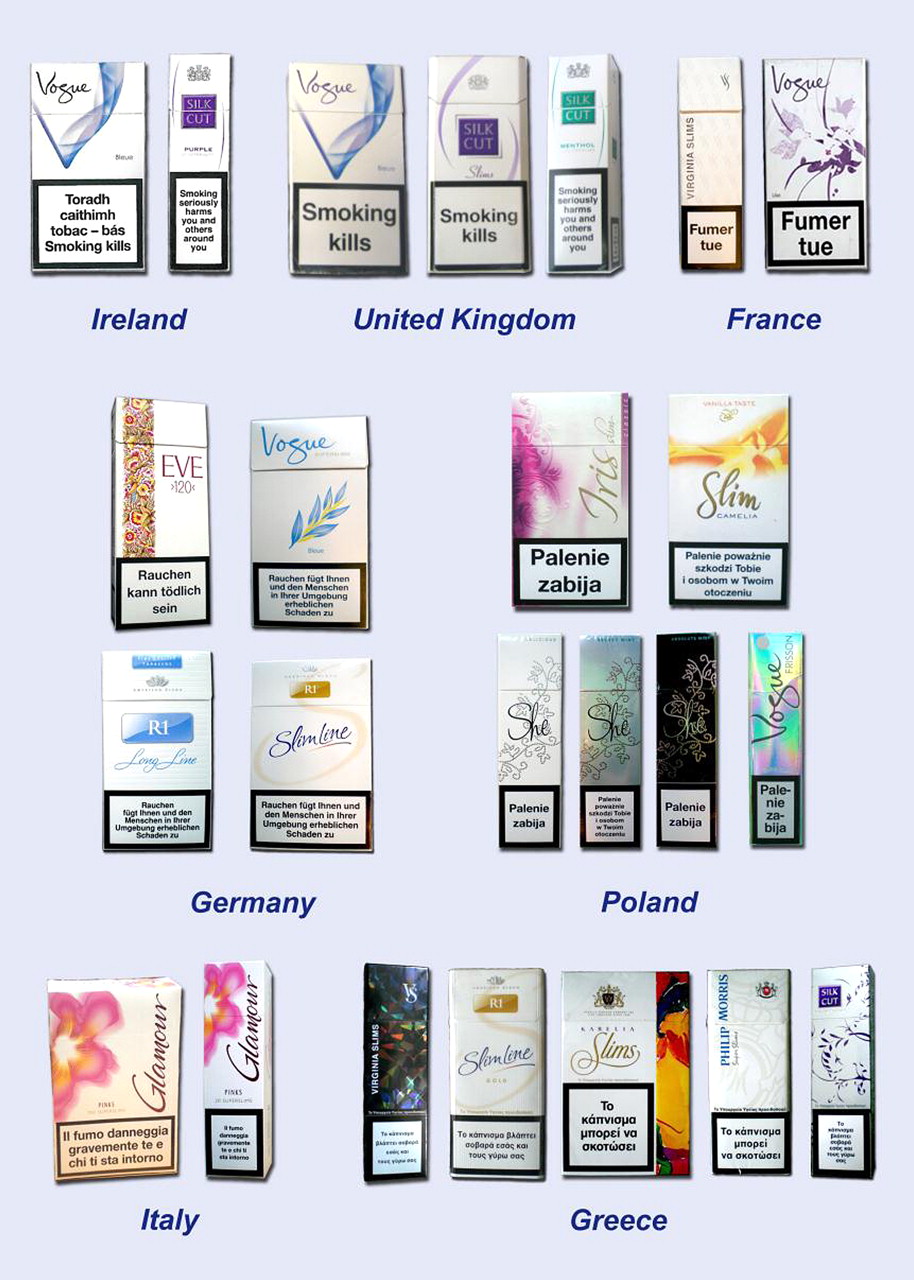
Cigarette brands, including slim and superslim versions, aimed at women in Europe.

Advertisement and examples of packaging for Vogue cigarettes in Russia.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Russian advertisements for Glamour Superslims on Moscow Metro, and advertising free gifts.
Linkages between modernity and smoking feature prominently in tobacco advertising. In the Philippines and South Korea, modernisation tends to narrow gender differences in youth smoking. Thus, continuing modernisation throughout Asia may increase smoking prevalence among young women, a pattern that is already evident in some countries.63 64 76 80 81 Indeed, tobacco companies adapt their marketing strategies to cultural contexts, including women's social and economic position in particular societies.63 76 82
A recent review of studies largely from HICs documented a causal relationship between tobacco advertising and promotion and increased tobacco use, as well as between exposure to depictions of smoking in movies and youth smoking initiation.83 This emphasises the importance of bans and restrictions on tobacco industry marketing, as required by the WHO Framework Convention on Tobacco Control (FCTC), to constrain the potential for growth in women's and girls' tobacco use in LMICs.
The impact of tobacco control policies on women and girls
In HICs tobacco control policies have had a major impact in reducing smoking prevalence, though these declines have not been equitable across population subgroups. There is evidence, mostly from HICs that elements of comprehensive tobacco control policies that reduce overall tobacco use can have different and sometimes more limited impacts among girls and women, particularly those of low SES.84
Price and taxation
Price increases reduce smoking prevalence and consumption in young people and adults.85 86 No consistent gender differences have been found among adults, however, a systematic review of US studies found young men were more responsive to price than young women.85 Studies in HICs find that low SES smokers are more price responsive than those of higher SES.86 However, in many LMICs, cigarettes are available by the single stick; thus increases in price and taxation may be less likely to have a significant impact since cost increases may not be as obvious to the user.
Smoke-free policies
Studies in HICs have found that where workplace policies are not comprehensive, low SES occupations such as the female-dominated hospitality industry are the least protected from SHS.65 In California, a US state which has comprehensive smoke-free legislation, low SES women reported higher workplace exposure to SHS, more exposure to SHS in the home and less control over home smoking policies than high SES women.87 Comprehensive smoke-free public places legislation can also encourage home smoking restrictions and reductions in children's exposure to SHS. However, this is not always the case; research in Scotland revealed that following the introduction of comprehensive smoke-free legislation, children's SHS exposure decreased in families where only the father smoked but not in families where only the mother smoked.88
Cessation support
In the UK, which offers free, comprehensive local cessation services including counselling and pharmacotherapy, women are more likely to use these services but have lower success rates than men.89 Quit rates are lowest in women who are younger, live in deprived areas and/or are from ethnic minorities.90 Local cessation services are generally unavailable in LMICs and access to pharmacotherapy is typically very costly.91
The lower smoking rates among women in LMICs are widely attributed to women's relatively poorer social and economic status and cultural factors rather than to the success of tobacco control.25 Indeed, tobacco control measures and policies vary enormously between LMICs and are generally poorly resourced.91 For example, tobacco control educational campaigns, typically underfunded—if available at all—in LMICs, rarely target sex or gender specific harms of tobacco use. Notably, strong evidence from several LMICs documents that women have low awareness of the health risks of smoking and have misconceptions about the harm of ‘light/low tar’ cigarettes. Studies in China, India, Indonesia and the Dominican Republic have found that while people (including health professionals) were generally aware that smoking is harmful they were less aware of specific health risks beyond cancer, particularly for those smoking at relatively low levels.90 92–95 One study in China found that over two-thirds of female smokers thought that ‘light’ or low tar cigarettes were less harmful than regular cigarettes,96 while another Chinese study found that awareness of ‘cigarettes made for women’ (women's brands) and believing that they were less harmful to health predicted smoking experimentation in female students.97 With regards to smoking during pregnancy, a study in Pakistan found that only 7% of women knew that smoking could lead to low birth weight; only one third of women knew that smoking caused lung disease.98 Similarly, a study in Zambia and the Democratic Republic of Congo found that pregnant women's knowledge of the health risks of smoking and SHS exposure was very limited.99 A study in South Africa found that over 45% of pregnant women who were smokers at the beginning of their pregnancy continued to smoke while pregnant. While most had some knowledge that smoking was harmful to their own health, they knew little about the impact of smoking during pregnancy.100 Additionally, in HICs and LMICs, insufficient attention has been paid to women's indigenous beliefs about smoking. In particular, the risk of having a low birthweight baby is often not a major concern for women, who may be unaware of the importance of normal birth weight, and may view quitting smoking as more stressful for the fetus than continuing to smoke.47 100
Incorporating gender and diversity-based approaches to tobacco control
In light of these analyses and trends, tobacco control strategies aimed at stopping and ultimately reversing the smoking epidemic in women need to be grounded in a multifaceted understanding of women's smoking patterns. This would take into account accelerated diffusion of cigarette smoking, gender inequities and gender relations, disadvantage and vulnerability to tobacco use. It would require more nuanced indicators of women's empowerment and emancipation and understanding of how gender intersects with other aspects of diversity such as social position, identity, ethnicity and religion.28 Given the lack of understanding of the harm of tobacco (particularly in LMICs), women-specific tobacco prevention education and cessation programmes need to be developed which clearly address misconceptions and local concerns.
Tobacco control therefore urgently needs to develop a more robust research base for developing such interventions for girls and women. In HICs, considerable research has focused on preventing and reducing tobacco use by women, especially pregnant women. In contrast, in LMICs, few studies have addressed women's tobacco use and SHS exposure.12 While it has been established that protective factors that operated in many LMICs, including cultural and economic constraints on women's smoking, are eroding because of globalisation and modernisation, little documentation exists on the woman-specific effects of these changes.
There is a need for quantitative and qualitative research at the individual, the community and the healthcare settings levels. Qualitative research methods, informed by gender and diversity considerations, such as participant observation, interviews and focus groups, would generate a deeper understanding of the complexity of social contextual forces which contribute to reported changes in women's tobacco use and SHS exposure in LMICs.12 Additionally, community-based participatory research in which community members work side by side with researchers to develop theory-based, culturally relevant tobacco control strategies, including policy approaches, would be useful. Community engagement fosters research and capacity building and has the potential to promote ownership and sustainability by mobilising communities to be active participants in tobacco control.
Applying a sex, gender and diversity based analysis to tobacco control research will enable measures, policies and programmes to be developed which are more salient to girls and women's lives, experiences and circumstances.1 4 6 28 101 For example, gender sensitive smoking prevention could help girls develop positive self-images and peer approval without cigarettes. Reassessing nicotine dependence measures such as the Fagerstrom test to take sex, gender, ethnic and ‘race’-related factors into account will improve treatment options for women and diverse populations.102 Multiple approaches are needed to denormalise tobacco use for women and girls. Health professionals in LMICs need training on the sex and gender specific health harms of tobacco, as well as gender sensitive skills training for approaching women about their tobacco use or exposure to SHS in every clinical encounter. In all countries, programmes should aim to empower women to reduce their exposure to SHS which may largely be from men's smoking.71 103 A smoke-free household initiative movement has begun in India and Indonesia. Although women in these countries involved in this movement initially expressed little self-efficacy to change smoking behaviour among men, they recognised, following culturally and gender sensitive health education on the harm of SHS, that a community-wide ban on household smoking might be effective. Now, Project Quit Tobacco International104 is fostering smoke-free homes, framing household smoking bans as an expression of collective responsibility and cultural pride. SHS is framed as a family health issue and an act of caring and being responsible for one's family.68
Gender sensitive approaches to reducing SHS in the home would recognise that in HICs exposure is greatest in low SES households, often led by women. Rather than increasing women's guilt and shame about exposing their children to SHS, a gender-sensitive approach would acknowledge women's desire to protect their children's health, and support them in coping with caring for their families in restricted circumstances while reducing SHS in the home.65 67 103
Conclusions
Increased female tobacco use poses serious threats to women's health, maternal and child health, and family health and economic well-being. The global picture of female tobacco use is increasingly complex, involving a range of tobacco products and responding to diverse factors including tobacco marketing, globalisation, urbanisation, modernisation and shifts in women's status and roles.105 The challenge for the 21st century is to prevent a further rise and reduce currently high levels of tobacco use by women, while ensuring that women's status continues to improve,1 101 requiring the WHO Framework Convention on Tobacco Control (FCTC) to animate its preamble's concerns with about women and tobacco, women's leadership in tobacco control and the importance of including gender analyses in tobacco control.7 Cultural constraints on women that might be protective against tobacco use should not be exploited or accommodated by tobacco control efforts, but rather transformed so that women's tobacco use can be reduced, and women's status improved at the same time.1 7 28 Organisations such as the International Network of Women Against Tobacco (http://inwat.org) are committed to these dual goals. Numerous reports and treaties such as The UN Convention on the Elimination of All Forms of Discrimination against Women (CEDAW)11 and the WHO FCTC support this dual approach to reaching their goals, which merits immediate adoption by the broader tobacco control movement.
What this paper adds
Tobacco companies are using gendered approaches to target girls and women.
However, gendered analyses and approaches to tobacco control research, policy and practice are uncommon, especially in low-income and middle-income countries.
This paper argues for gender and diversity analyses in tobacco control and illustrates how this should be used to reduce the impact of tobacco on women.
Acknowledgments
We thank Irina Morozova, Svitlana Sydorova, Magdalena Petryniak, Andriy Skipalskyi and Martina Pötschke-Langer for providing pictures of tobacco promotions and product. Amanda Amos is part funded by the UKCTCS, a UKCRC Public Health Research Centre of Excellence. Funding from British Heart Foundation, Cancer Research UK, Economic and Social Research Council, Medical Research Council, and the Department of Health, under the auspices of the UK Clinical Research Collaboration is gratefully acknowledged.
References
Footnotes
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.
Linked Articles
- Strategic directions and emerging issues in tobacco control
- Editorial