Article Text

Abstract
Background By 2030, the tobacco epidemic will be responsible for over eight million deaths worldwide per year, with 80% of those deaths occurring in low-resource countries. Despite the magnitude of the problem, little is known about the funding for global tobacco control.
Methods To estimate the amount of tobacco control funding, we created an integrated database based on information provided by tobacco control donors. We focus on resources available to low-income and middle-income countries provided as Development Assistance to Control Tobacco (DACT).
Results Global DACT grew from US$1.2 million in 2000 to US$44.2 million in 2009, primarily due to contributions from private philanthropies. Average annual 2000–2009 funding amounted to about US$0.003 per adult (US$0.0003 per adult in 2000 and US$0.011 per adult in 2009). DACT has been supplemented by domestic public funding that reached US$0.009 per adult in 2008. 28% of emerging and developing countries received zero DACT and 15% of those countries reported no funding at all. Out of US$21.8 billion disbursed in 2007 for health-related development assistance, DACT represented only US$0.02 billion, or 0.09%.
Conclusions Since the funding for both infectious and non-communicable diseases in low-resourced countries is inadequate, the solution for global tobacco control is not to shift resources from other public health priorities, but rather to generate additional tobacco control funding. Several mechanisms to achieve this goal are proposed.
- Tobacco control funding
- development assistance
- public policy
Statistics from Altmetric.com
Introduction
The tobacco epidemic is not only spreading, but its burden has been shifting from developed to developing nations.1 If the current trend continues, tobacco will kill more than eight million people worldwide every year by 2030, with 80% of those premature deaths occurring in low-income and middle-income countries.2 In addition, tobacco use imposes a substantial economic burden on both individuals and societies.1 ,3 Yet, investments in tobacco control are minuscule compared to other global health challenges, in both absolute and relative terms.4
Data on both domestic and international tobacco control funding are not readily available.4 Some attempts to determine the level of investment in tobacco control have been made, including one by the WHO Framework Convention on Tobacco Control (FCTC) Secretariat, but the conclusion was that this task is very difficult, if not impossible.5 ,6 The last conference of the Parties to the FCTC (Uruguay, 2010) requested the Secretariat to track tobacco control resources and to update them on a continuing basis.7 Publications such as Official Development Assistance (ODA) or Development Assistance for Health (DAH) do not include information about tobacco control funding.8 ,9 They reveal, however, that while non-communicable diseases pose a higher death burden than infectious diseases in developing countries, less than 3% of overall DAH in 2007 was dedicated to combating them.10 One study reported that the total amount available for development assistance in tobacco control was probably no greater than US$240 million in 2008,4 representing about 1% of DAH. Unfortunately, the methodology applied to generate this estimate was not described.
We have created a database of worldwide Development Assistance to Control Tobacco (DACT) in an attempt to estimate global tobacco control funding.
Background
During the 1980s and 1990s, small but crucially important funding for tobacco control in low-resource countries became available, primarily thanks to cancer charities based in the USA, UK, Canada, Australia and from the Union for International Cancer Control (UICC).11
Identified as a priority topic, tobacco control funding was discussed at the 9th World Conference on Tobacco or Health (1994), where the International Tobacco Initiative (ITI) was established in order to support research, knowledge management and tobacco control funding. ITI soon became Research for International Tobacco Control (RITC), disbursing about US$100 000 per year towards research, with funding coming primarily from the Canadian government.
In 2000 the American Cancer Society (ACS) and the Rockefeller Foundation began to invest in global tobacco control, which increased DACT to US$1 million that year, reaching nearly 40 countries. This amount doubled two years later, when George Soros's Open Society Institute (OSI) invested in tobacco control focusing on advocacy and networking between tobacco control advocates.
Since then, other organisations, both private and public, have stepped in to support global tobacco control. However, their contributions represent only a small share of their investment portfolio, leaving tobacco control in low-resourced countries underfunded and vulnerable. In 2004 the Rockefeller Foundation, which funded about 16% of DACT, discontinued its tobacco control funding in order to cope with stock market losses. In turn, the competition for global tobacco control funding intensified and many activities were put on hold.
A real breakthrough came in 2006, when Michael Bloomberg, encouraged by his success in tobacco control as mayor of New York City, announced his personal commitment of US$125 million to reduce the global burden of tobacco use. In 2008, Bloomberg Philanthropies increased this amount to US$375 million when the Bill and Melinda Gates Foundation joined the effort, investing US$125 million. The combined resources from these two private philanthropies amounted to US$500 million, to be invested from 2007 to 2013. This amount exceeded all previous development assistance for global tobacco control combined.
The historic shortage of funds and the relatively small number of entities funding global tobacco control motivated an effort to coordinate projects and to collaborate on funding for the larger ones. In 2002 RITC organised meetings to discuss such coordination as well as fundraising to support DACT. The meetings' participants identified a need to track the flow of global tobacco control funding, and OSI commissioned a feasibility study of such data collection. The study's results were presented in early 2006 to a group of tobacco control funders that formed the International Tobacco Control Funders Forum. The feedback from this informal group helped to shape the database when it became hosted by ACS in mid-2006.
In mid-2008, the database was reorganised with the goal of imposing a minimum reporting requirement on the participating agencies, while simultaneously capturing information of interest not only to the tobacco control community, but also to the global public health community. The database is now hosted by the International Tobacco Control Research Program (ITCR) at ACS.
Methods
We developed a measure for DACT by tracking contributions made by public or private institutions to tobacco control in 149 emerging and developing economies (online appendix 1).12 DACT includes funding for both country-specific and multinational projects, channelled through bilateral or multilateral donors, non-governmental agencies, private foundations and the corporate sector. We count annual disbursements rather than commitments made towards future payments and only those contributions absorbed by the targeted countries/regions. Therefore we do not include operating budgets of organisations that distribute funds. The database does not include projects with broad objectives that may (or may not) devote some amounts to tobacco control (eg, World Bank public health grants).
First, we identified organisations supporting global tobacco control by updating the list of funding agencies participating in the Funders Forum meetings. These agencies referred us to other organisations with potential interests in international tobacco control (a snowball method). If possible, the information in our database was first collected from publicly available sources (eg, annual reports, financial statements) and later verified by contacting a representative of the respective organisation. A standardised data collection form with agency-specific data was sent to all entities so they could verify the data and update them if necessary. The funders were asked to provide:
The title of the project being funded
The type of project (advocacy, institutional, research)
The type of funding (project-specific, general-operating, a mix of the two)
Whether the project was co-funded, and if so, the names of collaborating agencies
Country where the project took place
Name of institution receiving the funds
The total amount and currency in which funds were provided
The project's duration.
Advocacy projects are defined as activities aiming at influencing public policy or resource allocation. Institutional projects support the capacity of tobacco control agencies, and research projects advance scientific knowledge. In instances where a funder did not provide this information, we assigned the project type based on the title and/or description of the project. For eight projects the type could not be specified.
Project-specific funding supports a concrete activity and/or programme such as an advertising campaign. General operating funding adds resources that can be utilised even after the funding has ended, such as a purchase of equipment. Because of missing information we could not determine the type of funding for 49 projects.
We solicited information from 37 organisations in two waves of data collection in 2008 and in 2009. We received information from 30 organisations, which gave us a response rate of 81% (30/37) (see online appendix 2 for the list of participating agencies). Many organisations provided the data conditional on confidentiality about specific projects' amounts. Therefore, we only report aggregate data.
Since DACT can flow from primary funding sources through various intermediaries before it reaches an implementing institution, we checked all data to prevent double-counting and to eliminate other discrepancies and outliers. This allowed us to capture some data from non-participating organisations for projects that were co-funded with other agencies. The analysis was performed in Microsoft Excel 2003.
Our database contains data for 1995–2014. Since the information prior to 2000 was obtained retrospectively, we consider it less reliable. On the other hand, some funding committed for 2010–2014 had not yet been disbursed at the time of last data collection. Therefore, we decided to focus on the 2000–2009 time period, for which the data are most complete. Many commitments are for multi-year projects, thus yearly disbursements presented in this analysis can be lower than the total commitments, parts of which will be awarded in the future.
In addition to DACT, tobacco control funding can be provided by local governments. We used WHO data and referred to them as ‘domestic public funding’.2
DACT data were augmented by external country-specific data such as the gross domestic product (GDP), purchasing power parity (PPP),12 the size of the adult population (age 15+),13 the adult tobacco use prevalence13 and the exchange rates with respect to US$.14
Since the purchasing power of US$ (or donors' currency of choice) varies across countries, we adjusted funding amounts using PPP. The funding is then expressed in international dollars, which facilitates the comparison of funding level across countries. To distinguish between US and international dollars in this paper, we use ‘US$’ for US currency and ‘I$’ for international dollars.
Another way to compare the level of funding across countries is to express it relative to GDP level. For this purpose, we compared the 2000–2009 average amount of annual DACT to the average 2000–2009 GDP.
The geographical distribution of tobacco control funding is based on WHO regional classification: African region—AFRO, Region of the Americas—AMRO, Eastern Mediterranean region—EMRO, European region—EURO, South-East Asia region SEARO, Western Pacific region—WPRO. Thirty-three projects with unspecified geographical target were categorised as ‘multiregional’.
To distinguish between a one-time investment and a longer-term commitment for tobacco control, which is important for the effectiveness of tobacco control interventions,15 we created a variable that captures whether a country obtained more than one award between 2000 and 2009. We then calculated a sustainability index defined as the percentage of countries in each WHO region that obtained more than one disbursement.
Results
The database contains information on 956 tobacco control funding disbursements awarded from 1995 to 2010. Out of these, 893 DACT disbursements were awarded to emerging and developing economies between 2000 and 2009. This includes awards directed to individual countries as well as to multinational projects, amounting to US$132 million during this time period (or an average of US$0.003 per year per adult). The funding grew from US$1.2 million (or US$0.0003 per adult) in 2000 to US$44.2 million in 2009 (or US$0.011 per adult).
The field of global tobacco control is characterised by a high degree of collaboration among the funding agencies, since about 39% of awards were classified as collaborative.
There was almost an equal number of institutional (35%), research (32%) and advocacy (32%) projects funded between 2000 and 2009, but the value of funding favours research (US$47 million) and institutional support (US$43 million) over advocacy (US$36 million). The value distribution reflects the different cost structure of these project types (eg, research projects tend to be more expensive).
DACT went primarily to specific projects (82% of all awards and about half of money disseminated). About 14% of awards (and one third of the funding) contributed to the general operation of different organisations, and the remaining 4% could not be determined based on this criterion.
Geographical distribution of DACT
We were able to allocate funding to a specific WHO region for 97% of the awards. In nominal terms, the biggest amount was designated for WPRO and SEARO regions (26% and 19% of the total amount, respectively), but these two regions are also inhabited by more than half of the world's population. The smallest amount of total funding, about 4%, went to EMRO. About 23% of funds (or US$30 million) was spent across multiple WHO regions.
The intensity of DACT differs when evaluating tobacco control funding per adult. In this respect, the region with the most funding is AMRO, with more than twice as much as EMRO (figure 1). Even when the intensity of DACT increased substantially after the launch of the Bloomberg/Gates initiative, the relative order of WHO regions did not change, with the exception of WPRO, which moved from third to fifth place. The impact of the Bloomberg/Gates initiative on DACT is discussed below.
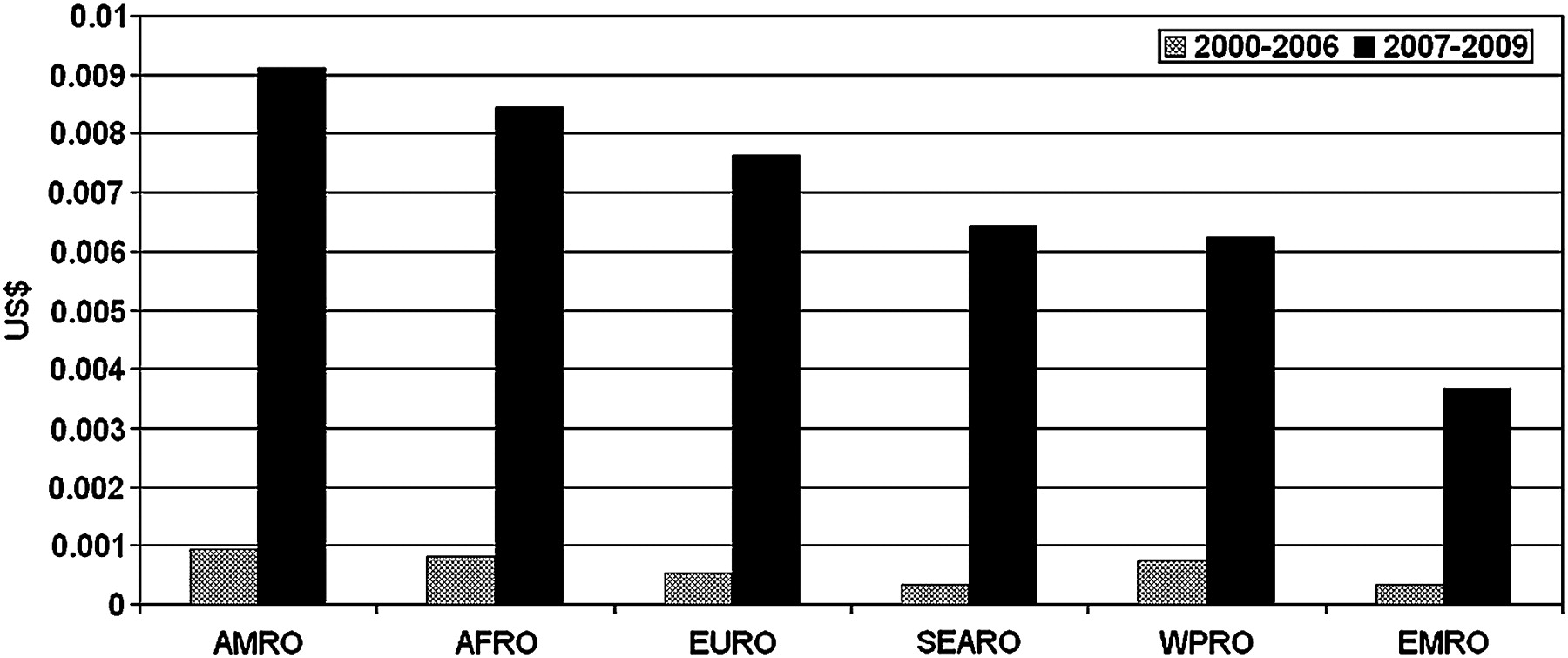
Average 2000–2006 and 2007–2009 annual DACT in US$ per adult in emerging and developing economies by WHO regions. Note: the figures do not include multiregional disbursements (about 23% of total funding) and apply to the population aged 15+ based on World Health Statistics.13
Other possible measures of DACT intensity are funding per person (including 0–15 age group) and funding per tobacco user. Using the former, AFRO falls behind WPRO and EURO. Using the latter, AFRO leads owing to relatively low tobacco use prevalence, but EMRO still occupies last place. Since tobacco control funds are also directed towards prevention, the per adult DACT presented in figure 1 seems the most appropriate measure.
About 80% of the 2000–2009 DACT value was designated for a specific country, reaching 72% of emerging and developing economies. The majority of DACT non-recipients are located in the AFRO and EMRO regions. Even though 45% of DACT non-recipients received some domestic public funding, this still leaves more than 15% of low-resourced countries with zero DACT and no reported domestic public funding.
In order to compare the 2000–2009 DACT level across individual countries, we converted the total country-specific awards into per adult (15+ years) annual DACT and expressed it in international dollars. The majority of countries received less then I$0.01 per adult annually. The highest per adult tobacco control resources (I$0.09–I$0.02) can be found in countries such as St Lucia, Jamaica, Barbados, Bahrain and Mauritius, owing to their small populations and the fixed costs associated with most tobacco control projects. Several countries in South-East Asia (Cambodia, Vietnam, Laos and Thailand) also received relatively higher per adult tobacco control funds (I$0.03–I$0.02), owing to the Rockefeller Foundation's investment. Funding over I$0.02 per adult also went to Lebanon and Uruguay. Twenty-one (20%) out of the total 107 emerging and developing economies with any DACT received less than I$0.001 per adult annually (see online appendix 3).
Another way to compare the level of funding across countries is to weigh tobacco control funds against GDP. DACT represents the largest share of GDP in countries with the lowest levels of economic development, such as Niger, Eritrea, Malawi, Cambodia and Laos. Other countries with a relatively high DACT to GDP ratio include Vietnam, Uruguay, Jamaica, Thailand and Georgia. But even in Niger, the country with the highest funding to GDP ratio, the DACT represents only 0.02% of the country's GDP (see online appendix 4).
The highest value of the sustainability index, about 60%, has been recorded in the AMRO and SEARO regions, meaning that 60% of the emerging and developing economies in those two regions were funded at least twice during 2000–2009. For AFRO, EMRO and EURO, the value of the sustainability index is slightly less than 50%. WPRO scored low on the sustainability with only about 30% of the countries receiving more than one disbursement during 2000–2009.
Domestic public funding for tobacco control
In addition to DACT, local governments and national institutions play an important role in funding tobacco control. The WHO data, mostly from 2008, revealed that this funding amounts to US$37 million (about I$73 million) in emerging and developing economies, or about US$0.009 (I$0.018) per adult per year.
Many countries still rely on DACT rather than on domestic funding, as DACT exceeded domestic public funding in 31 countries in 2008. In Mexico, for example, the government invested slightly more than I$25 000 into tobacco control in 2008, but the DACT reached nearly I$2 million in the same year. In Vietnam and Cambodia the DACT in 2008 was more than 10 times higher compared to domestic public funding. Sixty-three countries supported by DACT (59%) reported some domestic public funding. Globally, the 2008 DACT was higher than all domestic public funding combined ($US42 million vs $US37 million).
In Europe, domestic public investment in tobacco control is augmented by the European Union. We have obtained information on 30 grants disseminated by the European Commission between 2001 and 2008 valued over US$26 million (or US$3.3 million a year), but some of these grants were not solely directed towards tobacco control. In addition, only seven EU countries (representing about 17% of EU population) fall into the category of low-resourced countries. For that reason we do not include these grants in this analysis.
Bloomberg/Gates initiatives in global tobacco control
The Bloomberg Initiative, launched in 2006 and joined in 2008 by the Bill and Melinda Gates Foundation, changed the global tobacco control funding landscape (figure 2).

{kind=link}
{kind=link}
DACT in emerging and developing economies. Note: Includes only those awards on which information was obtained via our data collection effort.
Comparing 2000–2006 and 2007–2009 DACT, the average disbursement increased from US$86 000 to US$389 000 (by 352%). Not only were the awards larger after the launch of the Bloomberg/Gates initiative, they also increased in absolute numbers: during 2007–2009, funding was awarded 139 times per year on average compared to the yearly average of 68 disbursements in the previous period. The Bloomberg/Gates funding shifted focus from research and institutional support to advocacy. In previous years about 20% of disbursements supported advocacy projects (11% of awards' value), but starting in 2007 as much as 47% of the funding (28% of the awards' value) has been dedicated to tobacco control advocacy (table 1).
DACT before and after Bloomberg/Gates initiatives in global tobacco control
Discussion
The average worldwide DACT in emerging and developing economies amounted to US$13 million per year (or US$0.003 per adult) between 2000 and 2009, reaching US$44.2 million in 2009 (or US$0.011 per adult). Additional assistance from domestic public funds reached US$37 million in 2008 (or US$0.009 per adult).
WHO estimates that low/lower-middle-income and upper-middle-income countries need US$0.10—US$0.23 and US$0.11—US$0.72 per capita, respectively, in order to control the demand for tobacco.16 This estimate clearly contrasts with what is actually disseminated towards tobacco control in any emerging and developing country from DACT and domestic public funding combined. The tobacco control funding also contrasts with the tobacco companies' expenditures to promote their products. The industry spent over US$42 per capita on marketing tobacco in the USA in 2006, for example.17
Twenty-eight per cent of emerging and developing countries received zero DACT. With few exceptions, countries do not have funding for sustainable tobacco control interventions. Those exceptions are countries with strong civil societies or individuals who advocate for tobacco control, as they seem to attract and effectively utilise the funding (eg, South-East Asia Tobacco Control Alliance led by Bungon Ritthiphakdee, Witold Zatoński in Poland or Yussuf Saloojee in South Africa). This points to the importance of local leadership and strong civil societies. The Bloomberg/Gates initiative recognised this by funding the Global Tobacco Control Leadership Program at Johns Hopkins Bloomberg School of Public Health. OSI funding also supported civil societies. However, even strong local leaders and civil societies have to compete for limited resources, which can undermine the operation of existing and well functioning projects.
The funding from two private philanthropies (Bloomberg and Gates foundations) has changed the landscape of DACT by not only substantially increasing the resources available for tobacco control, but also by emphasising tobacco control advocacy. Did this influx of private funds encourage other organisations to enter the field to take advantage of possible synergies with the funded projects? Or were potential funders and local governments discouraged by feeling overshadowed by the size of this initiative (‘crowding-out’ effect)?18 ,19
The number of awards disseminated by organisations outside the Bloomberg/Gates initiative dropped after 2006. These organisations awarded 139 grants in 2005, but only 44 grants in 2009 (while there were 69 Bloomberg/Gates grants in 2009), with an overall 56% drop in the number of grants from other funders between 2007 and 2009. Some organisations—for example, Cancer Research UK, Atlantic Philanthropies, the Open Society Institute, even decided to drop DACT from their portfolio. This could be a sign of ‘crowding-out’. However, it could also be a reflection of the global financial crisis (2007–2009), which has weakened the budgets of many organisations. On the other hand, the organisations that remained in DACT kept increasing their commitments (in nominal terms) so that by 2008 the total value of their investment was 20 times larger compared to 2000. It is possible that the advocacy efforts funded mostly by the Bloomberg/Gates initiative have attracted additional funding for research and institutional support from other organisations fulfilling separate, but complementary needs in global tobacco control. However, we noticed a reduction in both the number and the value of awards by organisations outside the Bloomberg/Gates initiative in 2009 when compared to 2008, a possible effect of the global financial crisis. Longer time-series data are needed to determine whether a sudden influx of DACT from one or two donors had a negative effect on investments by other donors or local governments. If ‘crowding-out’ exists, then broader and long-term partnerships between donors and recipients, as well as increased transparency of funding, are needed to sustain financing levels. To nurture public domestic funding, external funders can provide the aid conditional on countries' commitments to keep tobacco control funding at certain level.20
Ideally, we would like to investigate the relation between DACT and tobacco use. However, such analysis on the global scale would be meaningless, since DACT is also directed towards the prevention of the tobacco epidemic. The relation between DACT and tobacco use can be studied in countries that are at the mature stage of the tobacco epidemic and have good data on both prevalence and funding over some period of time. Studies from high-income countries clearly demonstrate that investing into evidence-based tobacco control programmes leads to significant reductions in tobacco use among the targeted populations.21 ,22
Limitations
We believe that our database provides a good estimate of DACT spent in countries. However, despite our best efforts, we may have omitted some institutions funding tobacco control in countries of interest. In addition, broader funding for public health projects that could include tobacco control activities is not included in our database. Therefore, our estimate of DACT is conservative. We believe that our error is relatively small for two reasons: first, we collaborate closely with the global tobacco control community, which is characterised by a limited number of major funders; second, we obtained the data from all the key funders.
The data on domestic public funding also have their limitations, as they was self-reported in 2007 and 2008 by the WHO member states, with 38% of emerging and developing economies, inhabited by about 10% of the adult population living in these countries, not providing this information.
Even with these limitations, we can conclude that the level of funding for tobacco control is still substantially lower than funding for other public heath priorities, despite its high cost effectiveness.23–25 In 2007 about US$21.8 billion was disbursed for DAH in low-income and middle-income countries, of which US$5.1 billion was directed towards HIV/AIDS, US$0.7 billion towards tuberculosis and US$0.8 billion towards malaria.9 That contrasts with development assistance for tobacco control that, according to our data, reached US$0.02 billion in the same year (300 times less than the combined funding for HIV/AIDS, tuberculosis and malaria). Yet tobacco is responsible for over five million deaths,26 while HIV/AIDS, tuberculosis and malaria all together caused 4.4 million deaths in 2004.27
Conclusion
The funding for both infectious and non-communicable diseases in low-resourced countries is inadequate. The solution is not to shift funding among public health priorities, but to increase the total amount of funding. There are mechanisms that could increase tobacco control funding, but they are not used to their full potential. Article 5.6 of the FCTC calls for cooperation between the Parties to raise financial resources through bilateral and multilateral funding mechanisms. Other articles of the Convention provide more specific guidelines regarding financial resources (Article 20.5, Article 23.5 and Article 26).28 However, the mutual financial assistance among the Parties to FCTC has been very limited.29 Effective tobacco control programmes can complement programmes focusing on infectious diseases, as they would lower the number of premature deaths caused by infectious diseases (eg, smoking is a significant risk factor for tuberculosis).30
Private and public expenditures on tobacco control are overshadowed by the tax revenue governments receive from tobacco taxes. More than US$167 billion a year was collected in tobacco tax worldwide in 2008, yet less than 1% of this amount was devoted to curbing the epidemic.2 Governments also received at least US$10 billion in corporate income taxes from tobacco companies in 2008,4 with some receiving a part of the industry's profit in the form of dividends as well. In low-income countries only $1 out of US$9100 received in tobacco taxes was spent on tobacco control. In middle-income and high-income countries, this ratio was 1:4200 and 1:340, respectively.26 One way to improve this ratio is to specifically earmark a certain share of taxes collected on tobacco products for tobacco control, as has been done by some governments (eg, Thailand).
A necessary step to close the funding gap is to acknowledge tobacco control as a global health priority, which could help to locate additional resources within existing mechanisms across government structures and programmes in many advanced economies. For example, making tobacco control a signature US initiative on non-communicable disease within the Global Health Initiative could generate more DACT.31 Tobacco control could be also funded by new or existing global health partnerships (eg, Global Fund). A United Nations High Level Meeting on Non-Communicable Diseases, to be held in New York City in September 2011, creates an excellent opportunity to put tobacco control on the global public health agenda and to substantially increase resources for DACT.
Tobacco use presents an enormous and rapidly growing health burden worldwide. With the scarcity of resources and the irregularity of their distribution, tobacco control remains a global public health challenge. A compelling body of evidence demonstrates that the tobacco epidemic can be curtailed and many premature deaths can be avoided by implementing evidence-based tobacco control measures. Mobilising additional resources to fund these measures is imperative for both the tobacco control community and broader global health community.
What is already known on this subject
While tobacco use is currently responsible for at least 5.3 million premature deaths worldwide, little is known about the development assistance to address this global public health challenge.
What this paper adds
We have created an integrated database of worldwide Development Assistance to Control Tobacco (DACT) in order to provide an estimate of global tobacco control funding, to study its source, its focus as well as to point to the funding gap in low-resource countries.
Acknowledgments
We would like to thank Elizabeth Ward, Thomas Glynn, Wardie Leppan, Johanna Ralston and Judith Watt for their valuable comments, Deepa Naishadham for help with data visualisation and Alex Liber for editing assistance.
References
Supplementary materials
Web Only Data
Files in this Data Supplement:
Footnotes
Funding This study was supported by funding from the American Cancer Society and the Research for International Tobacco Control (RITC).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.