Article Text

Abstract
Background Previous studies showed reduction of hospital admissions for asthma after implementation of comprehensive smoke-free legislation. We aimed to evaluate the impact of comprehensive smoke-free legislation implemented in Hong Kong in 2007 on hospital admissions for childhood lower respiratory tract infection (LRTI).
Methods We obtained data on 75 870 hospital admissions for LRTI among children ≤18 years of age between January 2004 and December 2012 from all Hospital Authority hospitals. Using a negative binomial regression model, we assessed the impact of smoke-free legislation on admission counts.
Results After legislation implementation, there was an immediate effect with a change in the admission count of −33.5% (95% CI −36.4% to −30.5%), and a change in time trend to −13.9% per year (95% CI −16.0% to −11.7%). Overall, the legislation was associated with a net 47.4% reduction in admission counts in the first year. We estimated that the legislation was associated with a reduction of 13 635 admissions in the first 6 years after implementation. The immediate reduction and change in time trend was more apparent among school-age than preschool children.
Conclusions Implementation of comprehensive smoke-free legislation was associated with a significant reduction in hospital admissions for childhood LRTI.
- Public policy
- Secondhand smoke
- Environment
- Prevention
Statistics from Altmetric.com
Video abstract
Introduction
Substantial undisputable evidence has shown the adverse effects of environmental tobacco smoke (ETS) on respiratory morbidity and lung function in children.1 Children are more vulnerable because their lungs are still growing. Furthermore, they are inadvertently exposed to ETS from their parents smoking at home. Comprehensive smoke-free legislation has been implemented in several countries to reduce the harmful effects of ETS. However, there have been concerns about unforeseen consequences on children because it could force smoking parents to go back home to smoke2–4 though it was disputed by other studies.5 ,6 Recent studies have shown that smoke-free legislation was associated with a decrease in admission count for asthma in children and adults.7–9 Yet, few studies have reported on other respiratory outcomes besides asthma. Acute respiratory infection is the leading cause of death in children under 5 years of age and responsible for 1.6 million deaths globally each year.10 The causal relationship between ETS exposure and increased prevalence of lower respiratory tract infection (LRTI) in children has been well established.1 Nevertheless, only one previous study in adults11 and a recent study in children12 have investigated LRTI admission as one of the health outcomes of smoke-free legislation. In addition, all previous studies on the effects of the smoke-free legislation adjusted for seasonality, secular trends, etc, but did not adjust for the possible simultaneous effects of outdoor air pollution.9
To address these knowledge gaps, we aimed to assess the impact of the comprehensive smoke-free legislation implemented in Hong Kong (HK) in January 2007 on hospital admissions for childhood LRTI, which has been much higher than for childhood asthma. We also took into account the effect of outdoor air pollution, which has significantly increased in the past few decades in conjunction with the vibrant economic activities in the region. The findings from this study may provide more cogent evidence to support or dispute the impact of smoke-free legislation and the effects of air pollution on childhood LRTI, which will have important implications for healthcare policy.
Methods
Hospital admission data
The Hospital Authority (HA) hospitals receive over 90% of all hospital admissions in HK and the hospital fees are largely subsidised by the government.13 Since 1995, all HA inpatient data, including basic demographic characteristics, dates of admission and discharge, diagnoses and procedures on discharge using the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM), have been entered and stored on a central computerised database.14 Since HA holds strict rules and regulations for retrieving patient characteristics, we cannot request for home address which could be an indicator of socioeconomic status. We obtained data on daily unplanned hospital admissions for LRTI among children ≤18 years of age between January 2004 and December 2012 from all HA hospitals. On the basis of our previous study on the effects of air pollution and admission count for childhood asthma,15 the study period of 9 years should provide sufficient power to detect low correlations between air pollutants and admission count for childhood LRTI. We did not include the data in 2003 because the admissions were significantly affected by severe acute respiratory syndrome epidemics. We defined preschool as children aged 0–5 years and school-age as children aged 6–18 years. We defined admissions for LRTI as those with the following conditions as a principal diagnosis on discharge: acute tracheitis, acute laryngopharyngitis, acute bronchitis, pneumonia, pneumonia due to various types of organisms, bronchitis not specified as acute or chronic, empyema, pleural effusion, abscess of lung, with ICD-9-CM codes of 464.1, 464.2, 464.3, 464.4, 465.0, 466.0 to 466.1, 478.22, 478.24, 480, 482.0 to 482.2, 482.30–482.32, 482.4, 482.82–482.83, 483.0, 487.0, 486, 475, 490, 510.9, 511, and 513.0, respectively. We excluded admissions in which LRTI was not coded as the principal diagnosis.
Data on air quality and weather
The retrieval and handling of the data on air quality and weather followed our previous study.15 The data on sulfur dioxide (SO2), nitrogen dioxide (NO2), respirable suspended particulates defined as particulate matter with an aerodynamic diameter of 10 μm or less and 2.5 μm or less (PM10 and PM2.5),and ozone (O3) were obtained from the Environmental Protection Department.16 The data were collected from 11 stations that monitored general air quality and three stations that monitored roadside air quality across the territory. The hourly concentration record of each air pollutant from each included station was retrieved and the daily mean and IQR of each air pollutant was calculated. The arithmetic mean of each air pollutant from all included stations was also calculated. Meteorological data, including mean temperature, relative humidity and rainfall, were obtained from the Hong Kong Observatory.17 Pearson's correlation was used to determine the correlation between air pollutants and meteorological variables (see online supplementary table S1).
Lag times for the effects of weather
The effects of temperature, relative humidity, and rainfall on the day of hospital admission (lag 0) and up to 5 days before admission (lag 1, 2, 3, 4, and 5) were investigated and modelled using minimisation by Akaike's Information Criteria (AIC) and lack of overfitting or underfitting for the correction of residual autocorrelation. The mean daily temperature, relative humidity and rainfall were selected at different lag times for the best combined fit (see online supplementary table S2).
Data analysis
We used an interrupted time-series negative binomial regression model to assess the impact of smoke-free legislation and air pollution levels on hospital admissions for childhood LRTI. This model was similar to previous studies7 ,8 on the effect of smoke-free legislation on hospital admissions for childhood asthma. We chose negative binomial regression because this was shown to be a better model than Poisson regression for handling dispersion in time-series studies18 and it could estimate the immediate change and subsequent change in time trend after the implementation of the legislation.8 First, we input the daily hospital admission counts and meteorological data at different lag times for the best combined fit. We then included a dummy variable coded as 0 for the period before and 1 for the period after the legislation was implemented in January 2007 for the effect of the legislation. We also added a continuous variable set to 1 for 2007 through to 6 for 2012, which was equal to the respective number of years since the legislation took effect. These variables could address the immediate change and subsequent change in time trend after implementation of the legislation. We also input children's population counts for each year which were estimated by linear extrapolation of mid-year population estimates from the Census and Statistics Department.19 Other input variables included daily hospital admissions for influenza, each day of the study period to detect any secular trend, seasonal effects with a dummy variable for each month, and indicator variables for the day of the week and holidays. The effect of each air pollutant on the day of hospital admission and up to 5 days before admission was examined for potential delays in disease incidence after exposure. Multipollutant models were then run for pollutants that had significant effects in the single-pollutant analysis for the lag with the strongest effect. PM10 and PM2.5 were inputted separately in the multipollutant models due to their strong correlation. Using a χ2 test and AIC, we found that negative binomial regression performed better than Poisson regression. The test for non-linearity of the time trend with residual plots showed that the negative binomial regression gave an appropriate fit to the data.
We estimated the number of hospital admissions in the 6 years after the legislation had there been no legislation by using the β coefficients estimated in the model using all the data but setting the dummy variable to 0 for the time period after the legislation instead of 1 and removal of the continuous variable set for the 6-year period from 2007 to 2012. The number of hospital admissions prevented would be the sum of the differences in number of daily admissions between the actual admissions and the admissions had there been no legislation.
We then performed subgroup analysis using the same model except by inputting population counts for preschool/school-age subgroups instead of the whole population.
The effect of the smoke-free legislation was reflected by an immediate effect on hospital admission counts for LRTI of the 6-year period after versus the 3-year period before the legislation. In addition, the time trend after legislation was reflected by change in hospital admission count per year after the legislation. Both were expressed in percentage (with 95% CIs). The effect of the air pollutants was expressed as the percentage change (with 95% CI) in the daily hospital admissions with each increment or decrement of an IQR. All analyses were performed using SAS V.9.12.
Results
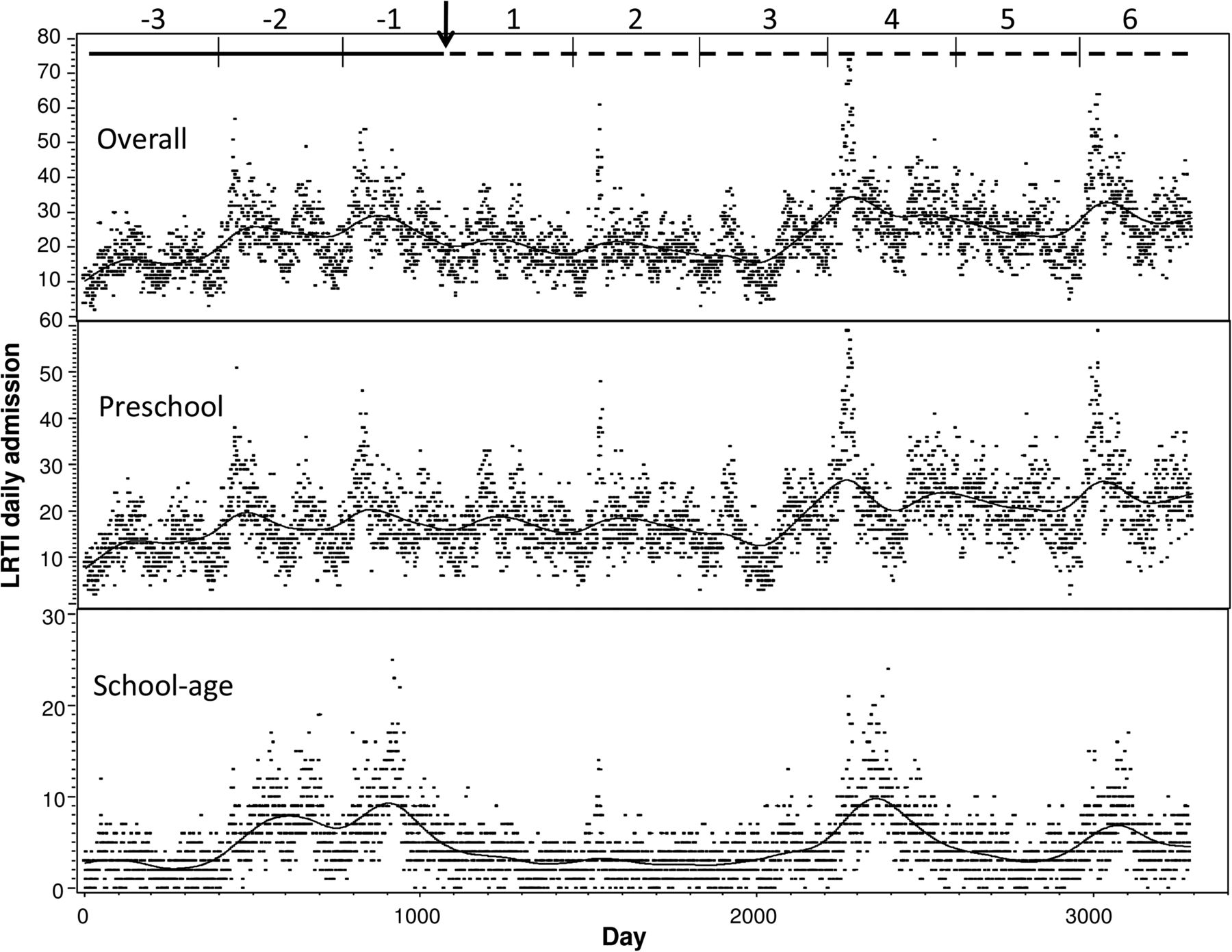
The data for hospital admissions, meteorological and pollution variables are summarised in table 1. Over the 9-year study period, there were a total of 691 480 hospital admissions (210 daily average), 75 870 LRTI admissions (23 daily average) and 16 178 influenza admissions (5 daily average) for children ≤18 years of age. Figure 1 shows the actual number of hospital admissions for LRTI among children ≤18 years of age over the study period.
Environmental variables and daily hospital admission data in children aged 0–18 years in Hong Kong between 2004 and 2012
{kind=link}
Hospital admissions for lower respiratory tract infection (LRTI) in children aged 0–18 years between 2004 and 2012.The horizontal solid line represents the years before the smoke-free legislation and horizontal dotted line represents the years after the smoke-free legislation; the vertical arrow represents the time at the implementation of the smoke-free legislation; the background dots are the actual hospital admission counts; the solid curve represents the spline smooth function of the mean hospital admissions for LRTI in children aged 0–18 years in the top panel, preschool children aged 0–5 years in the middle panel, and school-age children aged 6–18 years in the bottom panel.
There was no significant seasonal variation in ambient concentrations of PM10, PM2.5, SO2 and NO2. Ambient concentration of O3 was higher in the cold season (October–March) than in the warm season (April–September). PM10 was highly correlated with PM2.5 (r=0.92). The details of correlations among these meteorological variables are shown in online supplementary table S2.
The effects of smoke-free legislation on hospital admission for childhood LRTI with age-group analysis are shown in table 2. There was an immediate effect with a change in the admission count of −33.5% (95% CI −36.4% to −30.5%), and a change in time trend of −13.9% per year (95% CI −16.0% to −11.7%) after the legislation. Overall, the legislation was associated with a net 47.4% reduction in the admission count in the first year. We estimated that the legislation was associated with a reduction of 13 635 admissions in the first 6 years after implementation. In the age-group analysis, the reduction was more apparent among school-age children. There was a significant immediate change of −63.5% (95% CI −66.4% to −60.3%) immediately after the legislation and a change in time trend of −24.3% per year (95% CI −27.7% to −20.7%). In preschool children, there was a moderately significant immediate change after the legislation, but the change in time trend became less prominent with time.
Negative binomial regression model with multivariate analysis for the impact of smoke-free legislation on hospital admission count for lower respiratory tract infection (LRTI) in children aged 0–18 years between 2004 and 2012
The effects of multiple outdoor air pollutants (including PM10) on hospital admissions for LRTI with the age-group analysis are shown in table 3. Daily admissions for LRTI increased significantly by 6.7% (95% CI 4.3% to 9.1%) per IQR increase in PM10 (40 μg/m3) and by 7.3% (95% CI 4.7% to 10%) per IQR increase in O3 (37.5 μg/m3) on lag 1. On the other hand, there was a decrease of 2.4% (95% CI −3.7% to −1.1%) per IQR increase in SO2 (12.2 μg/m3) on lag 0. The effect of NO2 was not significant.
Daily percentage changes in daily hospital admission count for LRTI per IQR increase of the four pollutants in children aged 0–18 years between 2004 and 2012
Harmful effects from air pollutants were more apparent in preschool children, with an increase in daily admissions for LRTI of 7.9% (95% CI 5.2% to 10.8%), 3.4% (95% CI 1.4% to 5.4%), and 7.7% (95% CI 4.9% to 10.5%) per IQR increase in PM10, NO2 and O3, respectively. In school-age children, there was a significant increase in daily admissions of 5.2% (95% CI 4.9% to 10.5%) per IQR increase in PM10, but not for NO2 or O3. The results from the multipollutant model including PM2.5 are presented in online supplementary table S3.
Discussion
Our study showed that the implementation of comprehensive smoke-free legislation significantly reduced the hospital admissions for childhood LRTI. The immediate reduction in admission count and the subsequent change in time trend were more apparent among school-age children than preschool children. We estimated that the legislation was associated with a reduction of 13635 admissions in the first 6 years after the implementation. We also showed that outdoor air pollution levels were important risk factors for admissions for LRTI, especially in preschool children.
Despite the tremendous public health burden, acute respiratory infections are not generally recognised as a collective global threat, and far too little is being done to prevent or treat them.10 Although bacterial or viral agents are the cause of acute respiratory infections, there are well-recognised predisposing risk factors in children, such as poverty, malnutrition, overcrowding, pollution and exposure to ETS. Recent studies even showed a positive association between ETS exposure and increased severity of LRTI.20–22 However, only 14% of the world’s population live in countries or cities that have introduced comprehensive smoke-free legislation.23 A recent study in England shows that smoke-free legislation was associated with a large, immediate drop in LRTI admissions after smoke-free legislation but with no clear subsequent temporal rate change.12 In contrast, our study shows an immediate significant decrease in LRTI admission, as well as a sustained decrease in yearly count, albeit of smaller magnitude. The higher admission rate of 6–7 per 1000 children population for LRTI in HK as compared with 2–3 per 1000 children population for LRTI in England12 might partly explain the more sustainable effect observed in our studies. Our study adds new supporting evidence to accelerate the implementation or enforcement of smoke-free legislation worldwide, given the massive death toll and economic loss from tobacco-related death and sickness, particularly in developing countries where children are most vulnerable to such exposure.
In our study, the protective effect of smoke-free legislation on LRTI admission was more apparent in school-age children. One possible explanation is that smoke-free legislation forced smoking parents from public areas back home to smoke, as supported by the prevalence of self-reported exposure to ETS at home among primary school students has increased since the implementation of smoke-free legislation in HK.24 Since preschool children spend more time at home than school-age children, they may be exposed to more ETS and thus gain a comparatively smaller benefit from the legislation. Another possible explanation is that a significant proportion of preschool children during the study period were born to Mainland parents who were not residents in HK.19 Many of them were raised in Mainland China until they entered kindergarten or primary school, but would seek medical advice or be admitted to hospital in HK if they had a serious illness as they were entitled to the service. These preschool children would have had a much higher risk of exposure to ETS in Mainland China, where there was no smoke-free legislation; yet their hospital admission would be counted as if these children were residents of HK and there is no identifier in the HA database to exclude them from analysis.
Another important finding is the significant association between outdoor air pollution and admissions for childhood LRTI. Substantial evidence has shown an association between outdoor air pollution and admissions for asthma, especially in children,15 ,25 but the association of air pollutants, notably O3, PM10 and PM2.5, with admissions for LRTI is only emerging.26–29 Our findings provide additional evidences for the harmful effects of PM10, O3 and NO2, especially in preschool children. Although there have been some improvements in the levels of PM10 and PM2.5 in HK in recent years, the levels of NO2 and O3 have been steadily increasing. Our study results call for a more aggressive control of outdoor air pollution in HK. We found a decrease in admissions for LRTI with increased SO2 levels. This result was similar to our previous observation between SO2 levels and admission for childhood asthma.15 There could be unidentified confounding factors that account for this apparently incongruous finding, which warrants further investigation.
Our study has several strengths compared with similar studies. The computerised HA database has been in place for nearly 20 years. It is regularly audited, which reduces the classification bias of the health outcome. The relatively long observation period of 3288 days and a total of 691 480 hospital admissions provide an adequate power for the study. We have a dense population with detailed continuous monitoring of air quality. This allows a fairly accurate reflection of exposure to air pollution in our child population as a whole. Our novel study incorporated the simultaneous impact of smoke-free legislation and outdoor air pollution on admissions for LRTI in a single model. We also have a need to address the potential limitations, which were similar to other studies. First, the extent to which the legislation was enforced cannot be ascertained. Second, the ecological design precluded us from measuring any biological markers such as cotinine to delineate actual exposure to ETS. We cannot exclude the possibility that the adolescents smoked actively, but the self-reported smoking prevalence in youth was relatively low at 2.2% in our community.30 Third, we have not evaluated other factors that may have affected hospital admissions for LRTI during the study period, for example, introduction of universal pneumococcal conjugated vaccines in 2009, increase in children born to Mainland parents or territory-wide publicity campaigns to nurture a smoke-free culture in HK in the 1 year before legislation.31 Fourth, we did not adjust for socioeconomic status. Yet, we believed our result would not be significantly affected as >90% of our population uses HA in-patient service. Finally, we could not adjust for the time children spent in a different microenvironment as the variables were not available in the database.
Conclusions
The implementation of comprehensive smoke-free legislation in HK was associated with a significant reduction in hospital admissions for childhood LRTI, while outdoor air pollutants including O3, NO2 and PM10 continue to cause adverse effects on health.
What this paper adds
The association of the smoke-free legislation effect on asthma admission is shown in previous studies but its effects on other respiratory outcomes are uncertain. One notable example is lower respiratory tract infection (LRTI), which is an important cause of death in children globally. The evidences for the harmful effects of air pollution, notably particulate matter, ozone on LRTI, are also only emerging.
Our study demonstrates the smoke-free legislation effect on reducing children LRTI admission with immediate and sustainable effect. Overall, the legislation was associated with a net 47.4% reduction in the admission count of LRTI in children aged <18 years in the first year after the implementation of smoke-free legislation.
The study result also demonstrates the harmful effects of nitrogen dioxide in addition to particulate matter and ozone on LRTI admission in children.
Acknowledgments
The authors would like to pay a tribute to the late Professor Anthony Hedley and also thank Professor TH Lam for their significant contributions to the research work on combating air pollution and smoking in Hong Kong. They thank Dr Cheuk KL for his critical appraisal of the manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors SLL, WHSW and YLL jointly carried out the research. SLL wrote the first draft, with WHSW and YLL revised the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Ethics approval The study was approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster.