Article Text

Abstract
Objective Children are vulnerable to secondhand smoke (SHS) exposure because of limited control over their indoor environment. Homes remain the major place where children may be exposed to SHS. Our study examines the magnitude, patterns and determinants of SHS exposure in the home among children in 21 countries (19 low-income and middle-income countries and 2 high-income countries).
Methods Global Adult Tobacco Survey (GATS) data, a household survey of people 15 years of age or older. Data collected during 2009–2013 were analysed to estimate the proportion of children exposed to SHS in the home. GATS estimates and 2012 United Nations population projections for 2015 were also used to estimate the number of children exposed to SHS in the home.
Results The proportion of children younger than 15 years of age exposed to SHS in the home ranged from 4.5% (Panama) to 79.0% (Indonesia). Of the approximately one billion children younger than 15 years of age living in the 21 countries under study, an estimated 507.74 million were exposed to SHS in the home. China, India, Bangladesh, Indonesia and the Philippines accounted for almost 84.6% of the children exposed to SHS. The prevalence of SHS exposure was higher in countries with higher adult smoking rates and was also higher in rural areas than in urban areas, in most countries.
Conclusions A large number of children were exposed to SHS in the home. Encouraging of voluntary smoke-free rules in homes and cessation in adults has the potential to reduce SHS exposure among children and prevent SHS-related diseases and deaths.
- Secondhand smoke
- Surveillance and monitoring
- Global health
Statistics from Altmetric.com
Introduction
Exposure to secondhand smoke (SHS) from tobacco products is harmful to infants and children, and increases their risk of sudden infant death syndrome, more severe asthma, ear infections and respiratory infections.1–3 SHS exposure also can affect children's physical development, including their lung development.1–3 In addition, young children are uniquely vulnerable to SHS exposure because they have limited control over their environment.1
Advances in scientific knowledge on the dangers of SHS have raised awareness of the importance of protecting non-smokers from exposure through proven interventions, including smoke-free home initiatives.1–4 Acknowledgement of the dangers of SHS and the need to address the problem is reflected in the Guidelines on Protection from Exposure to Tobacco Smoke, which were adopted in support of Article 8 of the WHO Framework Convention on Tobacco Control (WHO FCTC), and which present best practices to eliminate SHS exposure in indoor environments.5 Article 8 calls on governments to promote effective measures to protect all people from exposure to tobacco smoke within 5 years of ratification, and it gives policy-makers a road map to achieve effective protection.5
According to the WHO,6 24% of low-income and middle-income countries (34 countries), by the end of 2014, adopted smoke-free policies that covered all public places such as work sites, bars, restaurants, schools, universities and healthcare institutions.7 ,8 Although smoke-free policies protect non-smokers from SHS in public places and stimulate adoption of similar rules in homes through normalisation of smoke-free environments, other measures may also be required to fully protect people from SHS exposure in non-public settings.9 ,10 These measures may include support for parents to change their attitude through education and counselling, smoking cessation support, a ban on tobacco advertising and increasing tobacco product taxes.11 ,12
Children's exposure to SHS in the home has been measured by studies that used cotinine as a biochemical measure of exposure. These studies found the presence of cotinine in children's blood serum and hair.13–15 Additional studies have assessed environmental markers of nicotine in homes occupied by children.14–16 For example, a cross-sectional study involving 31 countries measured air nicotine concentrations in households and cotinine concentrations in hair among non-smoking women and children in convenience samples of 40 households in each country.15 The study found that the dose–response relationship was more pronounced among children than among women. Moreover, air nicotine concentrations increased by an estimated 12.9 times in households that allowed smoking inside compared with those that prohibited smoking.
Research suggests that globally, an estimated 40% of children were exposed to SHS in any environment in 2004.16 However, a study that used Global Youth Tobacco Survey data from 132 countries collected during 1999–2005 estimated that 43.9% of youth aged 13–15 years were exposed to SHS at home.17 In the USA, a national study that measured participants' serum cotinine levels found that an estimated 40.6% of children 3–11 years of age had recent exposure to SHS.18 A study in Hong Kong found that 14.1% of students in grades 2–4 were exposed to SHS in the home.19 A study in the UK found a steady decrease in the proportion of children being exposed to tobacco smoke at home, from 37.0% in 1998 to 12.7% in 2012.13
While existing studies allow us to understand the magnitude of the problem and facilitate policy development, further evidence needs to be generated, particularly from low-income and middle-income countries where data are limited. Furthermore, data for these countries are important to aid in understanding the magnitude of the problem worldwide and to define tobacco control challenges, set priorities, guide solutions and monitor progress. This article seeks to reduce this knowledge gap by using data from the Global Adult Tobacco Survey (GATS) and population projections from the United Nations (UN) to estimate the proportion and number of children exposed to SHS in the home in 21 countries (19 low-income and middle-income countries and 2 high-income countries).
Methods
Data source
We used GATS data from 21 countries that conducted the survey during 2009–2013: Argentina, Bangladesh, China, Egypt, Greece, India, Indonesia, Malaysia, Mexico, Nigeria, the Philippines, Panama, Poland, Qatar, Romania, Russian Federation, Thailand, Turkey, Ukraine, Uruguay and Viet Nam. GATS was conducted in each country as a nationally representative household survey of people 15 years of age or older, to provide comprehensive information on tobacco use. A standard protocol is used for sampling, data collection, data management and weighting. This systematic collection of data allows researchers to monitor adult tobacco use and track key tobacco control indicators.20 Details of GATS methods have been published elsewhere.21 Sample sizes in the 21 countries ranged from 4359 (Malaysia) to 69 296 (India), and response rates ranged from 65.1% (Poland) to 97.7% (Russian Federation).
Measures
Presence of children in the home
GATS uses a household questionnaire and an individual questionnaire. The household questionnaire is used to collect information about household size, composition and family members’ tobacco use; the individual questionnaire is used to collect data from one randomly chosen member of each household who is 15 years of age or older.
The household survey uses two questions to collect information on the number of people in the household: ‘In total, how many persons live in this household?’; and ‘How many of these household members are 15 years of age or older?’. We computed the number of children younger than 15 years in each household by subtracting the number of people 15 years of age or older from the total number of household members.
Adult tobacco smoking
The household questionnaire also collects information about tobacco use among all household members. One household member who is 18 years of age or older is asked to list all household members who are 15 years of age or older who currently smoke tobacco, including cigarettes, cigars and pipes. If no household member is 18 years of age or older, a younger household member can answer this question.
Tobacco use was assessed on the individual questionnaire with the following question: ‘Do you currently smoke tobacco on a daily basis, less than daily, or not at all?’. We used responses to this question to estimate the proportion of households with an adult smoker in each country.
SHS exposure in the home
We used two questions to assess SHS exposure in the home. First, each respondent was asked, ‘Which of the following best describes the rules about smoking inside your home: smoking is allowed inside of your home, smoking is generally not allowed inside your home but there are exceptions, smoking is never allowed inside your home, or there are no rules about smoking in your home?’. Respondents who indicated that smoking was ‘never allowed’ inside their home were considered to live in a smoke-free home. Those who indicated that smoking was allowed inside their home or allowed with exceptions, were then asked, ‘How often does anyone smoke inside your home?’. Responses were categorised as ‘none’ (those who responded ‘never’) versus ‘some’ (those who responded ‘daily,’ ‘weekly’ or ‘monthly’). Those who responded ‘never’ were also considered to live in a smoke-free home and therefore not exposed to SHS at home. Those who indicated ‘daily’, ‘weekly’ or ‘monthly’, were considered to have been exposed to SHS at home.
Urban versus rural residence
The GATS sample design stratifies data by sex and residence (urban and rural) primarily to allow comparisons of estimates by these variables between countries.20 ,21 With the exception of Argentina, all countries in our analysis used a sample design stratified by residence.
Analysis
We examined the proportion of children younger than 15 years of age who were exposed to SHS in the home by country and by urban versus rural residence. Data for each country were weighted and calibrated to the national adult population. We used SPSS Complex Samples V.22 (IBM Corporation, Armonk, New York, USA) for data analysis. We calculated the weighted percentage of children younger than 15 years of age who were exposed to SHS in the home nationally, and by urban and rural residence. We calculated 95% CIs separately for each country. We also conducted a simple Pearson correlation between national SHS exposure prevalence estimates for children in the home and national smoking prevalence estimates for adults. In each country, we estimated the number of children exposed to SHS in the home by multiplying the prevalence from the GATS data by UN national population projections for 2015.22
Results
Table 1 shows that, among the 21 countries assessed, the proportion of children younger than 15 years of age who were exposed to SHS in the home ranged from 4.5% in Panama to 79.0% in Indonesia. Only two countries, Panama and Nigeria, had exposure prevalence estimates of <10.0%. When stratified by rural versus urban residence, the proportion of children exposed to SHS in the home was higher among those living in rural areas than those in urban areas, with the exception of Mexico, Romania and the Russian Federation.
Exposure to SHS in the home among children younger than 15 years of age, in 21 countries, by country and residence—GATS, 2009–2013
According to the UN population projections, approximately 994.80 million children younger than 15 years of age live in the 21 countries representing approximately 52.2% of world children in this age group. Of these, an estimated 48.7% (507.74 million children) were exposed to SHS in the home. Numbers ranged from 164.61 million in China to 38 000 in Qatar. The level of exposure in the following five Asian countries accounted for 84.6% of the children exposed to SHS in the home: China (164.61 million), India (162.14 million), Indonesia (57.72 million), Bangladesh (27.30 million) and the Philippines (19.00 million).
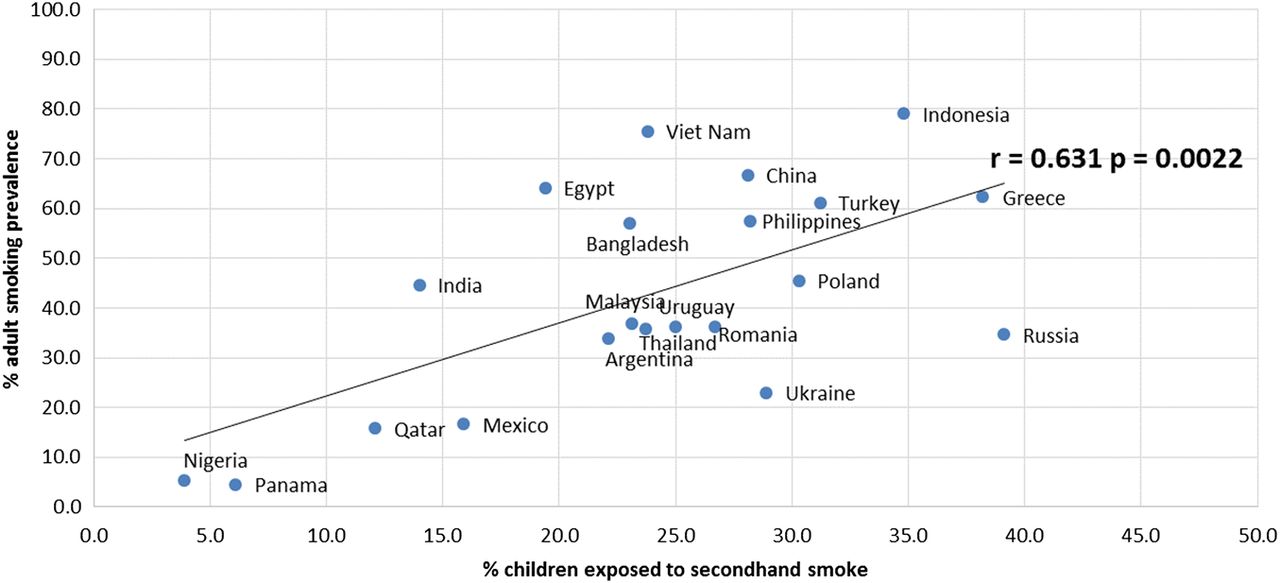
Countries with the lowest smoking prevalence among adults, such as Panama and Nigeria, generally had lower proportions of children exposed to SHS in the home (correlation (r) = 0.631) (figure 1). In contrast, countries with high smoking prevalence, such as Indonesia, Viet Nam and China, generally had higher proportions of children exposed to SHS in the home.
{kind=link}
Correlation (r) between children (younger than 15 years of age) exposed to secondhand smoke in the home and smoking prevalence among adults in 21 countries—Global Adult Tobacco Survey, 2009–2013.
Discussion
We characterised the prevalence of SHS exposure among children in 21 countries (19 low-income and middle-income countries and 2 high-income countries) and found that approximately one-half billion children were exposed to SHS in their homes. Countries with a high percentage of children exposed to SHS are more likely to experience a significant burden of SHS-related diseases and deaths. However, five countries—China, India, Indonesia, Bangladesh and the Philippines—that accounted for 84.6% of these children highlight the global magnitude of the burden of SHS exposure. People living in these countries may have a higher risk of diseases, death and disabilities that are associated with SHS exposure. Our findings underscore the importance of countries adopting the MPOWER policy package developed as part of the WHO FCTC as a way to protect people from SHS exposure through effective policies and programmes. The six components of MPOWER are: Monitor tobacco use and prevention policies; Protect people from tobacco smoke; Offer help to quit tobacco use; Warn about the dangers of tobacco; Enforce bans on tobacco advertising, promotion and sponsorship; and Raise taxes on tobacco.5 ,6 ,8 These policies and programmes are key to reducing smoking, and they also help create an environment that motivates people to quit tobacco smoking, which will in turn reduce SHS exposure among children.
Children may suffer disproportionately from SHS exposure, as they generally spend a significant amount of time at home.3 ,7 ,16 Children are also especially vulnerable because they have limited or no say on smoking in indoor places, particularly at home.3 ,7 In addition, their vulnerability may be exacerbated by a lack of medical and public health interventions, particularly in low-income countries.23 However, SHS-related diseases, death and disabilities in children are preventable,1 ,24 and evidence-based interventions, such as the adoption of voluntary rules for smoke-free homes, can be used to eliminate SHS exposure among children in the home.
Community education and awareness initiatives could also be used to increase knowledge and change attitudes about the health effects of SHS exposure, which could in turn increase the adoption of rules for smoke-free homes.25 ,26 These programmes could be promoted by healthcare providers, community leaders and other professionals who are in regular contact with families that have children. For example, the tobacco smoke-free homes initiative in Kerala, India, used this approach to reduce exposure to SHS, particularly among women and children in homes. The initiative developed by Project Quit Tobacco India engaged women's groups and community leaders in Kerala to raise consciousness about the dangers of SHS to non-smokers, particularly women and children, and to get support for a formal declaration for no smoking inside the home community. The initiative successfully increased the proportion of households with smoke-free rules in homes, from 20% to 60%.27
Our study found a positive correlation between adult smoking rates and SHS exposure among children in the home. This finding suggests that, in addition to promoting rules for smoke-free homes, efforts to reduce adult smoking could also help reduce SHS exposure among children in the home.7 ,25 Population-level efforts to further reduce adult smoking may include strategies such as increasing tobacco taxes and adopting smoke-free policies in public places.2 ,7 ,26 As the guidelines for Article 8 of the WHO FCTC indicate and evidence has shown, adoption of smoke-free policies in public places also has the potential to reduce SHS exposure in private homes.5 ,7 ,26 In particular, these policies can encourage a shift in social norms in which people begin to implement smoking restrictions in their own homes.7 ,26 ,28 In a study using GATS data from 15 low-income and middle-income countries, Nazar et al29 found a relationship between being employed in a smoke-free workplace and living in a smoke-free home. They found positive associations in all of the 15 countries studied (13 of the 15 being statistically significant) in individual-level country-specific analysis.
Our study also found that SHS exposure in the home was higher among children living in rural areas than those in urban areas in most countries. As people living in rural areas tend to have lower socioeconomic status (SES),30 ,31 this finding indicates that SHS exposure may disproportionately affect children with low SES.32 ,33 To address this disparity, tobacco prevention and control programmes in low-income and middle-income countries would need to ensure that smoke-free policies adopted and implemented also advance health equity.34 This is important, as some communities—particularly low SES communities, including rural areas in some countries—may not fully benefit from existing smoke-free policies due to inconsistent education and reinforcement of the policies.35 In this approach, it may be important to consider community initiatives to help raise awareness and support, and reinforce smoke-free policies.36 Engaging communities allows adoption of culturally appropriate strategies that help overcome some of the barriers to implementation of smoke-free initiatives. For example, the Project Quit Tobacco in Kerala, India, was able to get the communities to declare smoke-free homes through engagement of women and community leaders in raising awareness.27
This study is subject to at least two limitations. First, the potential for exposure misclassification exists because GATS does not use biochemical markers of inhaled smoke, such as saliva and urinary cotinine concentrations, to validate SHS exposure. However, past studies that compared self-reported exposure and biochemical markers have found these indicators to be strongly related.37 ,38 Second, variations in data collection times and changes in the strategies used to reduce SHS exposure in the 21 countries assessed restricted our ability to make comparisons between countries.
Despite these limitations, this study can help researchers understand the magnitude of SHS exposure among children in several low-income and middle-income countries. It also indicates that SHS exposure among children is high, especially in countries with high smoking prevalence and among rural populations. Implementing strategies to reduce SHS exposure, including the guidelines for Articles 8 and 148 of the WHO FCTC, could encourage adoption of voluntary rules for smoke-free homes and support cessation among smokers. Increased efforts to reduce SHS exposure in countries with large numbers of children could help to substantially reduce the harmful effects of SHS exposure among children across the world.
What this paper adds
Evidence has shown that children exposed to secondhand smoke (SHS) are particularly at risk of SHS-related diseases. Our study shows that about half a billion children in 21 countries (19 low-income and middle-income countries and 2 high-income countries), most of which have had limited evidence, are at risk of SHS-related diseases due to exposure at home.
Although countries with a high percentage of children exposed to SHS are more likely to experience a significant burden of SHS-related diseases and deaths, five countries—China, India, Indonesia, Bangladesh and the Philippines—that are home to the majority of the children exposed highlight the global magnitude of the burden of SHS exposure.
Acknowledgments
The authors thank Amanda Crowell, Technical Writer-Editor, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Atlanta, Georgia, USA, for substantial editing of the manuscript, and Edward Rainey, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Atlanta, Georgia, USA, for preparing the graph; and Jo Jewell and Julie Brummer, WHO Regional Office for Europe, for critically reviewing the final draft of the manuscript.
References
Footnotes
Collaborators GATS Collaborative Group.
Contributors LM made substantial contributions to conception and design, analysis, interpretation of data and writing of the manuscript. KMP made substantial contribution to conception and design, review and revision of the manuscript. LA conducted the data analysis for the manuscript. JM contributed to the design, review and revision of the manuscript. RB contributed to the design, review, analysis and revision of the manuscript. HF contributed to the review and revision of the manuscript in relation to the WHO Eastern Mediterranean Region. NR contributed to the review and revision of manuscript in relation to the WHO AFRO Region. RC contributed to the review and revision of the manuscript in relation to the Americas Region. RCD contributed to substantial review and revision of the manuscript in relation to the WHO European region. TMAW contributed to the review and revision of the manuscript in relation to the WHO European Region. DNS contributed to the review and revision of the manuscript in relation to the WHO South East Asia Region. MK contributed to the review and revision of the manuscript in relation to the WHO Western Pacific Region. ETd provided a World Health Organization critical review and perspective to the manuscript.
Funding GATS was supported by the Bloomberg Philanthropies’ Initiative to Reduce Tobacco Use, the Bill and Melinda Gates Foundation and the Ministries of Health in Greece, India, Malaysia, Panama, Qatar and Thailand.
Disclaimer The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention, World Health Organization or the governments of Argentina, Bangladesh, China, Egypt, Greece, India, Indonesia, Malaysia, Mexico, Nigeria, Panama, the Philippines, Poland, Qatar, Romania, the Russian Federation, Thailand, Turkey, Ukraine, Uruguay or Viet Nam.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Country Global Adult Tobacco Survey data sets used in this study are available online at CDC: http://nccd.cdc.gov/GTSSData/Ancillary/DataReports.aspx?CAID=2.