Article Text

Abstract
Objectives This study examined the effect of pictorial health warning labels (HWLs) on the waterpipe (WP) device on smokers’ experience, puffing behaviour, harm perception and exposure to respiratory toxicants.
Methods Thirty WP smokers completed two 45 min ad libitum smoking sessions (WP without HWL vs WP with HWL) in a crossover design study. Exhaled carbon monoxide (eCO) was measured before and after each smoking session. Puff topography was recorded throughout the smoking session, and participants completed survey questionnaires assessing subjective smoking experiences and harm perception.
Results Significant differences were observed in eCO levels between the two study conditions, with lower levels of eCO boost recorded following smoking the WP fitted with HWL (16 ppm) compared with WP without HWL (22.7 ppm). Participants had more puffs, shorter interpuff intervals and a higher total puff volume during smoking the WP without HWL relative to WP with HWL (p values <0.05). We documented enhanced reports of satisfaction, taste and puff liking following smoking the WP without HWL compared with the WP with HWL. WP harm perception was significantly higher among participants after smoking the WP with HWL compared with WP without HWL.
Conclusion This pilot study shows that placing HWL on the WP device is effective in reducing WP smoker’s positive experiences, puffing parameters and exposure to carbon monoxide. HWLs lead also to more appreciation of WP harmful effects, making them a promising regulatory approach for addressing the spread of WP smoking among young adults in the USA.
- smoking topography
- prevention
- toxicology
Statistics from Altmetric.com
What this paper adds
This is the first clinical laboratory study to provide evidence of the effect of placing pictorial health warning labels (HWLs) on the waterpipe (WP) device.
Placing pictorial HWL on the WP device is effective in reducing WP smoker’s positive experiences, puffing parameters and exposure to carbon monoxide.
The regulatory and policy implication of such results are strong and call for the consideration of placing pictorial HWLs on WP devices.
Introduction
Waterpipe (WP) smoking (aka hookah) has become popular in the USA, particularly among young people.1 According to national data from the Population Assessment of Tobacco and Health Study (2013–2014), WP smoking was only second to cigarettes in 18–24 year olds, with 18.2% of them reporting current WP use.2 Evidence shows that WP smoking can lead to dependence and many of the known smoking-related diseases.3 4 Recognising the seriousness of the WP epidemic, regulatory bodies including the Food and Drug Administration (FDA) recently have extended their authority to include WP products.5 However, evidence to guide effective regulatory and policy efforts to curb WP spread among young adults is still underdeveloped.6
One feature underlying WP’s popularity among young adults is the widespread misperception of ‘reduced-harm’ compared with cigarettes, which is mostly due to a belief about the ‘filtering’ effect of water in the WP device.7 This misperception has been exploited by WP-related industries that emphasise in their marketing efforts the health and safety of their products.8 Thus, communicating actual harms related to WP smoking represents a promising avenue to curb WP use in the USA and protect public health.
Health warning labels (HWLs) communicate evidence-based risk information that can correct misperceptions of a safe product and have been a principal strategy for reducing tobacco use globally.9–12 Cigarette HWLs have been shown to raise awareness about smoking harms, prevent initiation and encourage smoking cessation.13 However, similar evidence regarding the effect of HWLs on WP smoking is lacking. Recently, the WHO released a report recommending placing HWLs on WP devices, especially at WP cafés.14
Beginning in 2018, the FDA will require that WP tobacco packages have a textual HWL: ‘WARNING: This product contains nicotine. Nicotine is an addictive chemical’.4 While this HWL represents a good first step, it is inadequate given the established harm of WP smoking beyond nicotine exposure and the superior performance of pictorial HWLs over text-only HWL. In addition, the WP café is an important component of WP spread among youth and should be considered in any HWL-related policies .6 15 Available evidence from the USA shows that between 37% and 44% of current WP users smoke it in the café,16 17 where consumers are usually not in contact with the tobacco packaging and thus would not see the FDA-mandated HWL. Furthermore, WP smokers have the most extended contact with the device, not the tobacco, during prolonged WP smoking sessions averaging an hour. In a recently published study involving focus groups and in-depth interviews with WP smokers and non-smokers, the WP device was identified as the optimal location for HWLs.18 Therefore, developing WP-specific HWLs, and involving other WP components (eg, device), is expected to be a promising option for regulatory and policy bodies interested in addressing the spread of WP among young people.
Recently, we have started developing WP-specific HWLs as part of an National Institutes of Health-funded project (1R01TW010654-01). In this proof of concept study, we used two of the developed prototype HWLs in a clinical lab setting to examine if fitting the WP device with pictorial HWLs influences smokers’ experience, puffing behaviour, harm perception and exposure to exhaled carbon monoxide (eCO).
Methods
Participants
Thirty participants were recruited from Miami and its surrounding metropolitan area by placing flyers around WP venues (hookah cafés and bars). Participants were healthy WP smokers who smoked at least 1–3 WPs per month in the past 6 months. Participants were between the ages of 18 years and 30 years and provided informed consent for study participation. Exclusion criteria included self-reported history of chronic health problems or psychiatric conditions, regular use of prescription medications (other than vitamins or birth control) and self-reported current use of >5 cigarettes or other tobacco/nicotine products in the past month. Women were excluded if they were breast feeding or tested positive for pregnancy (by urine pregnancy testing) at screening. Participants were preliminarily screened on the phone for potential eligibility and the information was later confirmed during an in-person screening session.
Procedures
All participants completed two smoking sessions (WP without HWL vs WP with HWL, figure 1), preceded by ≥12-hour tobacco/nicotine abstinence confirmed by eCO <5 ppm and separated by at least 48 hours (washout period to avoid carryover effects). For the HWL condition, we applied two randomly assigned graphic variants and their corresponding text: (1) ‘WARNING Using the charcoal to heat the hookah produces a chemical that causes cancer’ and (2) ‘WARNING Chemicals in hookah cause cancer’ (figure 1). During each session, the WP head was filled with 15 g of the participant’s preferred tobacco and covered with perforated aluminium foil.16 Preferred brands were Al Fakher (United Arab Emirates; n=28) and Starbuzz (USA; n=2). Participants smoked the same brand and flavour in both conditions. The HWL was placed in a constant location/size on the WP device and was placed in front of the participant’s seat at eye level. Tobacco was heated with quick-light charcoal disks (35 MM Coconut Shell Instant Light charcoal; Starbuzz Tobacco). The charcoal brand was held constant across participants and conditions. For standardisation, only one type of WP device was used (Khalil Mamoon 27’’, Egypt). Participants were instructed to smoke the WP ad libitum for up to 45 min. eCO was measured before and after the WP session.16 Subjective responses were assessed after the smoking session. During each session, participants were seated in a reclining chair and were given the choice to watch movies while smoking. Payments were provided to compensate for participants’ time, effort and expense of attending sessions.16

Illustration of the WP devices with HWLs (first condition) and no HWL (second condition).
Measures
Subjective measures
Participants responded to three self-administered subjective measures: The Duke Sensory Questionnaire (DSQ), The WP Evaluation Scale (WES) and a harm perception measure.16 Below are additional details about these measures.
WES is an 11-item questionnaire that was adapted from a similar scale used for cigarettes19 20 (by replacing the word ‘cigarette’ with ‘waterpipe’). This scale assesses participants’ perception of the smoked WP (eg, satisfying, tastes good and makes you dizzy); each WES item was rated on a 7-point Likert scale (‘not at all’ to ‘extremely’).
DSQ has nine items that assess participants’ sensory experience of the inhaled product (eg, How satisfying were the puffs?); all questions were rated on a 7-point Likert scale (‘not at all’ to ‘extremely’).21
Harm perception in this study was assessed using a two-item scale adapted from previous literature.22 These were (1) ‘In your opinion, how harmful is the WP to general health?’ and (2) ‘In your opinion, how harmful is smoking cigarettes for health?’ The answers to both were rated on a seven-point scale ranging from 1 (not at all harmful) to 7 (extremely harmful).
WP smoking topography
Smoking topography was assessed using a validated WP topography instrument developed by the American University of Beirut.23 24 Briefly, a WP hose was fitted with a differential pressure flow meter. Inhalation-induced pressure changes were amplified, digitised and sampled using an automated data acquisition system. The topography software converted pressure signals to air flow (mL/s) and integrated the flow data, producing measures of total smoking time, total puff time, puff duration, interpuff interval (IPI), number of puffs, total volume inhaled and average puff volume.
Exhaled carbon monoxide
Measurements of eCO were recorded before and after WP use via BreathCO monitor (Vitalograph, Lenexa, Kansas, USA).
Data analysis
Descriptive statistics for the characteristics of the study sample were summarised as means and SDs or proportions, as appropriate. Means were calculated for all outcome measures (ie, measures of smoking topography, eCO and subjective experience items) and compared by session (WP without HWL vs WP with HWL) using two-tailed paired samples t-tests. For eCO measures, eCO boost was calculated by subtracting the presession measurement from the postsession measurements.25 To compare the effects of HWL condition on eCO concentration, data were entered into a repeated model ANCOVA with two within-subject factors: time (presmoking and postsmoking session) and HWL condition (WP without HWL vs WP with HWL). Huynh-Feldt corrections were used to adjust for potential violations of the sphericity assumption.26 In this analysis, we controlled for gender, age of initiation of WP smoking and number of WPs smoked in the past month, as these are expected to influence smoking patterns and reflect on eCO.27–29 Significance was set at p<0.05. All analyses were performed in IBM SPSS V.21.30
Results
Study participants (n=30) had a mean age of 21.5 (SD=2.6) years and ranged from 18 years to 30 years. Participants were mainly males (n=23; 76.7%). Eighteen participants (60%) self-identified as white, eight as African-American/black (26.7%) and four as other (13.3%). The mean age for starting smoking WP was 17.4 (SD=2.4). The mean eCO level at screening was 2.1 ppm (SD=1.6). See table 1 for full details of participant characteristics.
Baseline characteristics for the overall sample (n=30)
WP smoking topography
Statistical analysis results for the puff topography data are shown in table 2. Significant differences were observed between the two conditions for the following topography measures; smoking time, puffing time, IPI, total volume and puff volume. For each of these items, values were greater after smoking the WP with no HWL (p values <0.05) compared with WP with the HWL condition. The greatest difference detected was for the puff volume and the total volume inhaled. For example, the total amount of smoke inhaled in the HWL condition was on average 23.9 L less than in the no HWL condition (p<0.05).
Waterpipe smoking topography measures by no health warning label (HWL) and HWL conditions (n=30)
Exhaled carbon monoxide
A large effect size31 (partial eta square ηp 2=0.14) for time by condition interaction was observed for eCO concentration (F=4.8, p<0.05). This means that changes in eCO levels across time depended on the HWL condition. Mean eCO concentration for the no HWL condition increased from 1.08 ppm (SEM=0.2) presession to 24.5 ppm (SEM=4.2) postsession resulting in an overall change of 22.7 ppm (SEM=4.2). For the HWL condition, the mean eCO concentration increased from 1.8 ppm (SEM=1.2) presession to 17.8 ppm (SEM=21.7) postsession resulting in an overall change of 16 ppm (SEM=3.9). eCO boost (post–pre) was less in the HWL condition compared with no HWL condition (p<0.05; figure 2).

Means (±SEM) for exhaled carbon monoxide levels presession/postsession by HWL condition (n=30). HWL, health warning label; WP, waterpipe.
Subjective measures
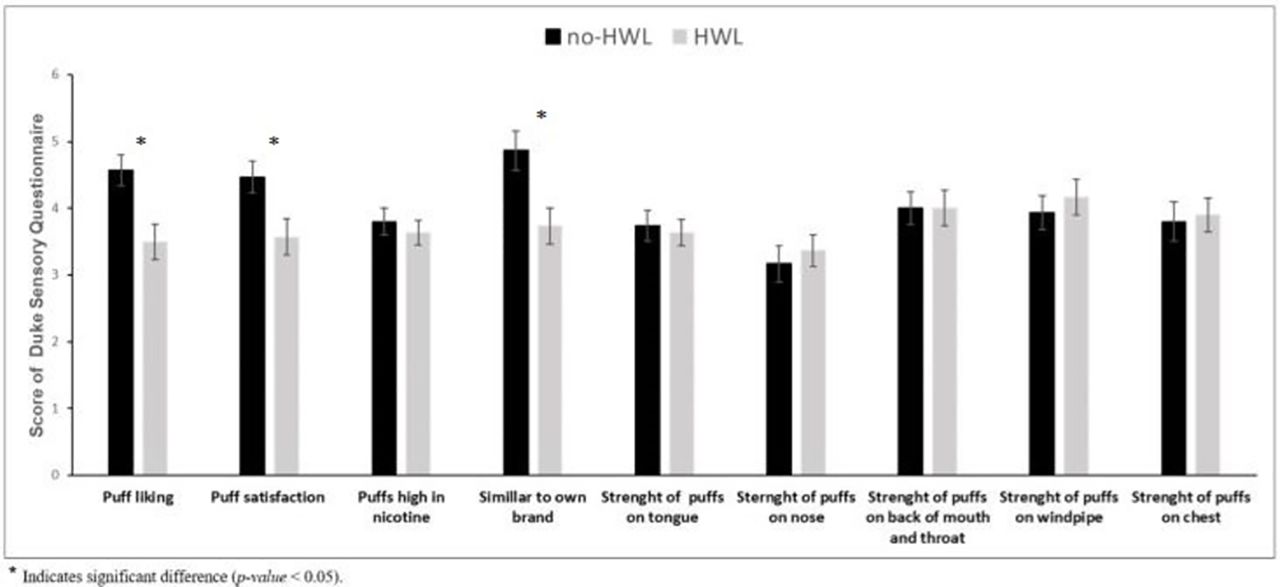
Subjective measures also showed important differences between the two conditions. Figures 3–5 depict mean postsession ratings for WES, DSQ and harm perception for the two conditions, respectively. For the WES, significant differences were observed according to condition for the following measures: ‘Was it satisfying?’ and ‘Did it taste good?’ (figure 3). For each of these items, values were greater after smoking the WP with no HWL compared with the WP with HWL (p values <0.05). The greatest difference detected was for feeling satisfied after smoking. Means for all other subjective measures of WES were greater in the no HWL condition, except feeling nauseous, and the ability to curb craving, which were greater in the HWL condition (p>0.05). For the DSQ, significant differences were observed between conditions for the following items: ‘How much did you like the puffs?’, ‘How satisfying were the puffs?’ and ‘How similar to your own brand/flavor were the puffs?’ (figure 4). For each of these items, values were greater after smoking the WP with no HWL compared with the WP with HWL condition (p<0.05). The greatest difference detected was for the similarity of product to the smoker’s own brand.

Means (±SEM) for postsession subjective responses for the WP Evaluation Scale by HWL condition (n=30). HWL, health warning label; WP, waterpipe.

Means (±SEM) for postsession subjective responses for the Duke Sensory Questionnaire (n=30). HWL, health warning label.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
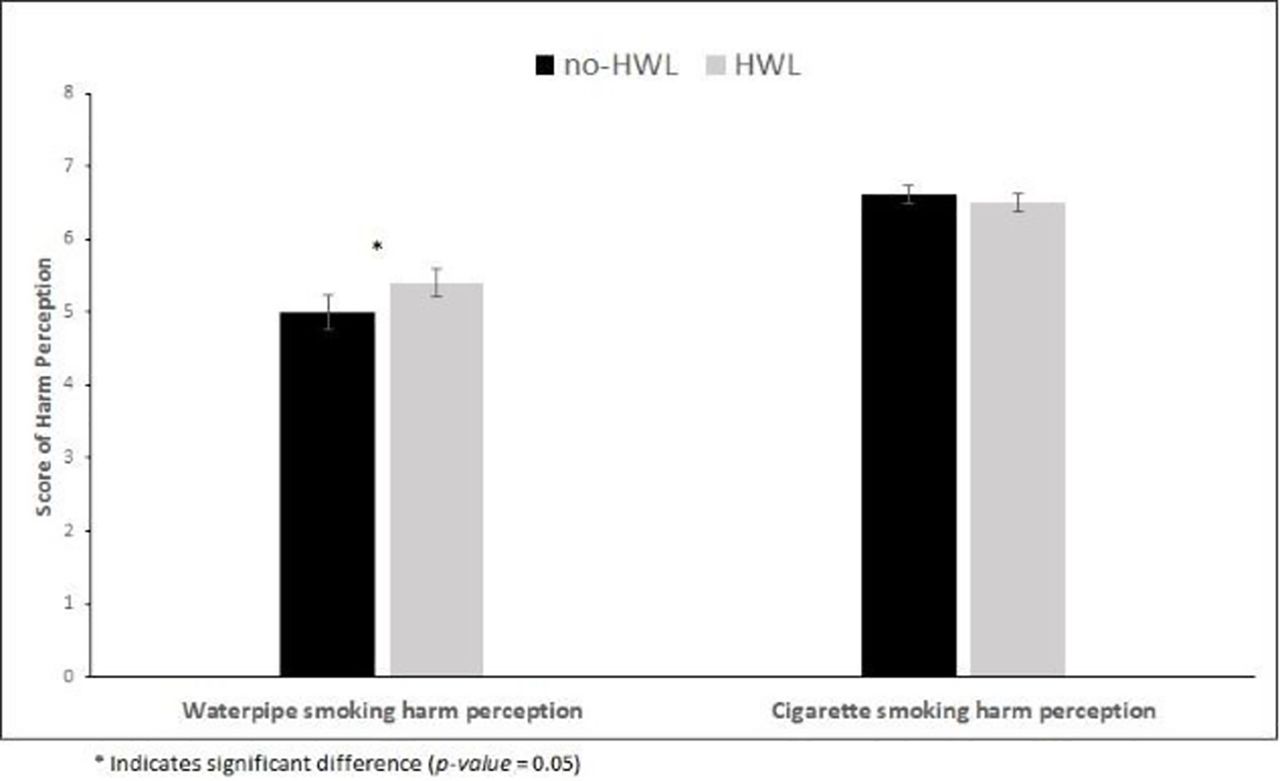
Means (±SEM) for postsession harm perception responses by HWL condition (n=30). HWL, health warning label.
In addition, there was a significant difference for harm perception towards WP smoking, as participants reported higher perception of harm following smoking the HWL condition compared with the no HWL condition (p=0.05). There were no significant differences in harm perception among participants towards cigarette smoking (figure 5).
Discussion
This clinical laboratory study is the first to provide a proof of concept that including a HWL on the WP device is effective in reducing WP smokers’ positive experiences and exposure to eCO. Our results showed attenuated puffing behaviours as a result of smoking WP fitted with the HWL, which likely underlie the observed difference in eCO exposure and suggest a reduction in smokers’ exposure to a variety of other respiratory toxicants. Furthermore, smoking WP with HWL increased smokers’ awareness of the potential harm of WP smoking compared with no HWL. Taken together, these results show that placing HWL on the WP device is an effective and promising strategy to reduce WP appeal for young adults, their smoking experience and exposure to smoking-related toxicants and to increase their perception of the harms associated with WP smoking. The evidence from this study provides a consistent picture across a variety of subjective and objective measures of the effect of HWLs on the WP device on WP smokers. All the documented effects were in the direction of reduction of positive and increase in negative experiences associated with WP smoking with the addition of HWL compared with no HWL.
Our results show that fitting the WP device with HWL led to less intensive puffing behaviours and accordingly less exposure to eCO. The 21.5% decrease in eCO boost in the HWL condition compared with control is indicative of HWL potential for harm reduction. While it is hard to predict the long-term effect of such decrease in exposure on WP-related health effects, the main value of HWLs lies in motivating smokers to quit and discouraging nonsmokers from initiation.32 As for the smoke volume differences, we noticed on average 24 L decrease in the total smoke inhaled during the HWL session compared with control. To put that into perspective, in an average cigarette smoking session smokers inhale about 0.5 L of smoke.28 33 Also, smoking time was on average 4 min less in the HWL condition compared with no HWL.
The main goal of using HWLs is to communicate smoking-related risks, influence risk perception and induce behaviour change.32 We could document an effect on harm perception in this study, as participants smoking the WP with the HWL perceived WP smoking as more harmful compared with smoking the WP without HWL. Our results are consistent with existing evidence from the cigarette literature that highlights the effectiveness of HWLs in increasing risk perception and knowledge regarding the harmful effects of smoking.32
While our study provides novel insights into the potential of HWL on the WP device for WP regulation and policy, our results should be considered in the context of the study limitations. This study involved a sample of 30 young participants from the Miami metropolitan area (mostly college students), which can limit its generalisability. Also, the study was not powered to detect differences in outcome measures between the two HWLs used and did not include a broader arsenal of important outcomes for HWLs research, such as the intention to quit. Therefore, future larger studies are needed to assess differences between different HWLs and their representative themes (eg, health risks to self vs others). These studies might also include a broader assessment of outcomes. Obviously, we could not blind participants to the study conditions and general purpose, but they were blinded to the specific hypotheses to be tested. Also, the order of the two sessions was not counterbalanced, but there was at least 48 hours gap between the two sessions that minimises any carryover effect.34 Moreover, the laboratory environment unavoidably differs from the typical WP smoking atmosphere, which usually involves social interaction and WP sharing.35 We tried to minimise this effect by equipping our lab with a reclining chair, offering participants the opportunity to watch movies of their choice and allowing them to access their mobile phones. Future studies can look at how group WP smoking, which is common in WP cafés, may be affected by HWLs and whether it changes the social atmosphere around the WP and prompts discussion of health effects. Still, for a proof of concept study, the study sample and measures provided strong and consistent evidence about the potential of HWL on the WP device as a promising regulatory and policy strategy.
This study is the first to provide clear and consistent evidence of the potential of pictorial HWLs on the WP device to reduce positive smoking experiences, puffing parameters and exposure to CO while increase negative experiences and harm perception among young WP smokers. The regulatory and policy implication of these results are strong and support the consideration of placing pictorial HWLs on WP devices in addition to the tobacco packaging. Given that the WP smoker has the longest contact with the WP device and that within the popular WP café setting exposure to HWL on the device can be augmented by other WPs with HWLs in the venue, the WP device seems like an optimal location for effective HWLs to curb the spread of WP smoking among young adults in the USA and beyond.
References
Footnotes
Contributors WM, ZBT and MEK conceptualised and designed the study, supervised data collection, performed the initial analyses, contributed to interpretation of the data and drafted the initial manuscript and critically revised the manuscript for important intellectual content. TE, JT, AS and TA contributed to interpretation of the data and critically revised the manuscript for important intellectual content. All authors read and approved the final manuscript.
Funding This study was supported by the National Institute on Drug Abuse/Food and Drug Administration (FDA) award R01 DA042477 and Fogarty International Center (FIC) award R01 TW010654. TE and AS are funded, in part, by the National Institute on Drug Abuse of the National Institutes of Health under Award Number P50DA036105 and U54DA036105 and the Center for Tobacco Products of the US FDA.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the views of the NIH or the FDA.
Competing interests None declared.
Ethics approval This study was approved by Florida International University Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.