Article Text

Abstract
Objectives To investigate the links between health warning labels (WLs) on cigarette packets and relapse among recently quit smokers.
Design Prospective longitudinal cohort survey.
Setting Australia, Canada, the UK and the USA.
Participants 1936 recent ex-smokers (44.4% male) from one of the first six waves (2002–2007) of the International Tobacco Control 4-Country policy evaluation survey, who were followed up in the next wave.
Main outcome measures Whether participants had relapsed at follow-up (approximately 1 year later).
Results In multivariate analysis, very frequent noticing of WLs among ex-smokers was associated with greater relapse 1 year later (OR: 1.52, 95% CI 1.11 to 2.09, p<0.01), but this effect disappeared after controlling for urges to smoke and self-efficacy (OR: 1.29, 95% CI 0.92 to 1.80, p=0.135). In contrast, reporting that WLs make staying quit ‘a lot’ more likely (compared with ‘not at all’ likely) was associated with a lower likelihood of relapse 1 year later (OR: 0.65, 95% CI 0.49 to 0.86, p<0.01) and this effect remained robust across all models tested, increasing in some.
Conclusions This study provides the first longitudinal evidence that health warnings can help ex-smokers stay quit. Once the authors control for greater exposure to cigarettes, which is understandably predictive of relapse, WL effects are positive. However, it may be that ex-smokers need to actively use the health consequences that WLs highlight to remind them of their reasons for quitting, rather than it being something that happens automatically. Ex-smokers should be encouraged to use pack warnings to counter urges to resume smoking. Novel warnings may be more likely to facilitate this.
- Cessation
- packaging and labelling
- public policy
- addiction
- environmental tobacco smoke
- end game
- older people and smoking
- advertising and promotion
- health communication
- media campaigns
- qualitative study
- public opinion polls
- smoking topography
- population health
- nicotine reduction in cigarettes
- tobacco products
Statistics from Altmetric.com
- Cessation
- packaging and labelling
- public policy
- addiction
- environmental tobacco smoke
- end game
- older people and smoking
- advertising and promotion
- health communication
- media campaigns
- qualitative study
- public opinion polls
- smoking topography
- population health
- nicotine reduction in cigarettes
- tobacco products
Introduction
Health warning labels (WLs) on cigarette packets have consistently been shown to have beneficial effects.1 ,2 They provide information, raise awareness of smoking-related risks,3–5 promote quit-line use,6 ,7 reduce cigarette packet appeal,8 strengthen intentions to quit9 and increase cessation behaviours such as reducing cigarette consumption10 ,11 and making quit attempts.12 Never-smokers report that WLs help discourage them from taking up the habit.13 Among experimental adolescent smokers, WLs can reduce intentions to smoke and lead to forgoing of cigarettes.14 The impact of WLs for ex-smokers, however, is not well understood. An early evaluation of large text-based warnings indicated that recall of warning messages among ex-smokers did not continue to increase as it had among smokers, presumably due to lack of continued exposure to the warnings among the former.15 When asked, however, ex-smokers retrospectively cited WLs as having motivated them to quit.16 Around one-third of surveyed ex-smokers reported that WLs are also effective in stopping them from smoking,5 and among those quit for <1 year, over half reported that WLs help them stay quit.13 We are not aware, however, of any prospective studies looking at the impact of reactions to WLs on preventing relapse.
Risk of relapse decreases the longer a smoker has been quit17 and with greater self-efficacy to remain quit,18–20 but increases with greater exposure to other smokers in the home, social or professional settings17 ,21 ,22 and with greater nicotine dependence,21 ,23 ,24 particularly reported frequency of strong urges to smoke.17 Experienced benefits of smoking also predict relapse, albeit mediated by reduced self-efficacy and increased urges to smoke.17 However, research has failed to find effects of perceptions of harms of smoking as protecting against relapse.25 WLs may provide a mechanism for making the harms of smoking salient enough at the time of crisis to counteract competing tendencies to smoke (ie, relapse). If WLs have any effect, it would be by making these issues salient at the appropriate time.
Research with smokers has shown that a more in-depth level of processing of WLs, beyond mere noticing (like reading them or thinking about their meaning), is required to encourage thoughts about quitting and forgoing cigarettes.12 Smokers' avoidance of warnings is also positively associated with subsequent quitting.12 Perhaps paradoxically avoidance too is indicative of deeper processing of WLs, as it indicates a strong negative affect towards the idea of smoking causing harm, and if the belief is strong enough, the only means of fully resolving it is to quit. It is likely, therefore, that if WLs can also help ex-smokers to stay quit, it would involve some sort of active engagement with the warning stimuli, for example, to help generate reasons for resisting the temptation to smoke. We theorise that these reactions are part of a process of conferring negative affect to smoking and producing impulses to refrain. These affective reactions can be triggered by recall of beliefs about the harms of smoking. The stronger these affective tendencies, the more likely they will exceed the strength of the urge to smoke and stimulate quitting activity. Once a quit attempt is initiated, the strength of these negative affective reactions to smoking will be an important deterrent to relapse, in a context of fluctuating strength of urges to smoke.
The International Tobacco Control 4-Country policy evaluation project (ITC-4) commenced in 2002 to monitor the impact of tobacco control policies. It is a longitudinal cohort study that annually surveys smokers from Australia, Canada, the UK and the USA, which all have different labelling policies: Canada has required graphic warnings covering 50% of the front and 50% of the back of cigarette packets since December 2000 and was the first country to do so. From 1995 to March 2006, Australia required text-only warnings to cover 25% of the front and 33% of the back of packets, after which it implemented graphic warnings covering 30% of the front and (with added text information) 90% of the back of packets. In September of 2002, the UK implemented large text-only warnings covering 30% of the front and 40% of the back of packets, prior to which it only required text warnings on 6% of the front of packs.i The USA requires small text-only warnings on the side of cigarette packets, which fail to meet the standards of the Framework Convention on Tobacco Control (FCTC) and have been in place since 1984.ii
The present research uses data from the ITC-4 to determine the extent to which ex-smokers notice WLs and whether WLs are associated with a lower likelihood of relapse. The relationship between measures of reactions to health warnings and relapse are likely to be complex. Recent ex-smokers will likely try to minimise their exposure to cigarettes as much as possible. Thus, mere exposure to the warnings, because it entails concurrent exposure to cigarettes, is likely to be positively associated with relapse. If we control for this, however, then we expect that processing of the warnings will be protective.
Method
Data collection and sample
Participants were ex-smokers (quit <1 year ago), who provided outcome data approximately 1 year later. The data source was waves 1–7 (2002–2009) of the ITC-4-Country project, which only recruit's smokers but retains those who subsequently quit (including between recruitment and the initial full survey, typically conducted a week or more later). Standardised telephone interviews were conducted annually, with an intake of new smokers at each wave to replenish numbers lost to attrition (around 30% per wave). Smokers and ex-smokers received different versions of the survey. For more details, see Thompson et al 26 and also http://www.itcproject.org/research.
Only participants who reported being quit during one of the first six waves were of interest for the present study, and the flowchart in figure 1 details the selection criteria. The final sample comprised N=1936 participants taken from waves 1–6 of the survey, of whom 57.5% were still quit at the follow-up wave (waves 2–7). An additional 1007 participants who met the baseline eligibility criteria were lost to follow-up. They did not differ from those retained in the study on sex, socioeconomic status, heaviness of smoking index (HSI) scores while smoking, frequency of urges to smoke, residual perceived benefits of smoking, self-efficacy to stay quit, baseline quit length or frequency of noticing WLs. However, participants lost to follow-up were significantly younger, t(1894.9) = 6.8, p<0.01, more likely to be from the USA or UK, χ2(3) = 32.1, p<0.001, were more likely to report that WLs make you ‘a lot’ more likely to stay quit, χ2(3) = 15.4, p<0.01, have more friends who smoke, χ2(5) = 18.5, p<0.01, be more likely to live with other smokers, χ2(1) = 10.0, p<0.01, notice more pro-smoking media, χ2(1) = 11.2, p<0.001, and be more likely to report that WLs had prevented them from smoking while a smoker, χ2(1) = 4.2, p<0.05. These measures were all included in our final model. The first survey during which participants reported being quit will be referred to as their ‘quit baseline’ wave. This was not normally their first main wave of participation, occurring on average 647 days (SD=72) after recruitment. At the time of their quit baseline survey, the average time that participants had been quit for (their ‘baseline quit length’) was 129 days (SD=106).

Flowchart of selection criteria, missing data and valid sample sizes for analysis. *Note: some key questions relating to warning labels (WLs) were not asked in wave one, accounting for much of the missing data (model 4 was particularly affected by this, as it also assessed responses to WLs in the wave prior to quit baseline). Participants for whom quit baseline occurred in wave 7 were also excluded, as wave 8 data were not yet available. See text for further details.
Variables of interest and analytical procedure
Three variables relating to cigarette packet WLs at quit baseline were of interest: “In the last month, how often if at all, have you noticed the warning labels on cigarette packages (Never, Rarely, Sometimes, Often, or Very often)?”; “To what extent, if at all, do the warning labels make you think about the health risks of smoking (Not at all, A little, Somewhat, or A lot)?” (both validated in relation to quitting activity12 ,15) and a new measure “To what extent, if at all, do the warning labels on cigarette packs make you more likely to stay quit (Not at all, A little, Somewhat, or A lot)?”.
A series of binary logistic regression analyses were conducted to predict smoking status (relapsed or still quit) at follow-up. All were adjusted for age, sex, socioeconomic status (education tertiles and annual household income tertiles combined), country of residence and baseline quit length (transformed using a natural logarithmic function17). We also controlled for a number of other covariates, which fell into three broad categories:
-
Exposure to tobacco-related cues (measured at quit baseline): the number of smokers among participants' five closest friends, number of smokers in the home, whether smoking was allowed at home and the frequency of noticing pro-smoking material in the media (radio, billboards and shops).
-
Other predictors of relapse17 (measured at quit baseline): frequency of urges to smoke, level of self-efficacy to remain quit and a measure of residual perceived benefits of smoking (smoking is an important part of life, helps to reduce stress and is too enjoyable to give up for good).
-
‘While-smoking’ covariates (measured approximately 1 year prior to quit baseline): the HSI derived from the number of cigarettes smoked per day and minutes to first cigarette after waking,27 the frequency of noticing WLs while smoking, whether WLs ever stopped the participant from having a cigarette while a smoker15 and to what extent WLs made the participant more likely to quit while a smoker (all missing participants for this question, 19.4%, were included as a separate valid category).
Unless otherwise acknowledged, all measures were created or adapted by the ITC team. For any categorical or ordinal variables, dummy variables were created for each category for use in regression analysis. The simple associations of all key variables and covariates were first examined, adjusted only for demographics and baseline quit length. The effects of the covariates were then systematically explored using a cumulative strategy. Model 1 looked at the combined effects of the WLs, adjusted for demographics and baseline quit length, model 2 controlled for all covariates in model 1 plus exposure, model 3 controlled for all covariates in model 2 plus the other known predictors of relapse and model 4 controlled for all covariates in model 3 plus the while smoking covariates.
Results
Summary sample characteristics are presented in table 1, where some country differences are apparent. Participants from the UK and USA were older than those from Australia and Canada, F(3, 1932)=29.4, p<0.001, there were relatively more UK residents coded into the low socioeconomic bracket, χ2(6)=55.2, p<0.001, and the level of nicotine dependence (HSI) among Australian participants (and to a lesser extent those from the USA) was lower than among Canadians and those from the UK, χ2(18)=57.1, p<0.001.
Summary characteristics of participants by country
Reporting that WLs make you more likely to stay quit was strongly correlated with reporting that WLs make you think about health risks (r=0.63, p<0.001). Given this high correlation, it was decided to exclude WLs make you think about health risks from the multivariate analyses reported here. The simple associations controlling for demographics and time quit at baseline (table 2, first column) show that greater noticing of WLs was associated with greater relapse but reporting that the warnings help to stay quit was protective. Not shown in this table, reporting that the health warnings lead to thinking about the health risks of smoking was not significant in the analyses of the contributions of the individual variables. This column also shows that the influences of the other predictors of relapse were in the expected directions, and time quit at baseline was strongly associated with relapse.
Predictors of relapse at 1-year follow-up, including demographics, exposure, known predictors and reactions to warning labels (WL) while quit
In the multivariate modelling, very frequent noticing of WLs remained a significant predictor of relapse when the combined effect of the two WL questions were analysed together, indeed both effects were stronger (model 1). The effect of noticing declined marginally when measures of exposure to smoking were included (model 2), with number of friends who smoke being positively associated with relapse. The effects of noticing became non-significant after controlling for known predictors of relapse (model 3). Reporting a relapse preventive effect of the warnings remained relatively stable across these analyses. The estimated probability of relapse among participants reporting that WLs made them a lot more likely to stay quit was 0.41 compared with 0.50 among those who said not at all when we adjusted for all covariates included in model 3 (the unadjusted rate of relapse for the whole model 3 sample was 0.43).
We also conducted a number of further analyses that are not detailed here.iii First we controlled for measures of health warnings and HSI at the previous wave (while still smoking) where the data were available (‘model 4’, see figure 1), and this had no additional effects except that noticing the warnings while smoking predicted relapse and the non-significant effect of noticing while quit reduced further. Next we only included cases (n=1088) who reported any noticing of the warnings at quit baseline and recomputed models 1–3. Noticing was not significant in any model and the effect of reporting a protective effect of the warnings was stronger, OR=0.55 (95% CI 0.38 to 0.79). We next investigated five theoretically plausible interaction effects. These were baseline quit length with frequency of noticing warnings and also with WLs make you more likely to stay quit, frequency of noticing WLs with frequency of urges to smoke and with self-efficacy to stay quit and self-efficacy with WLs make you more likely to stay quit. None of these interaction effects, however, were statistically significant in predicting relapse.
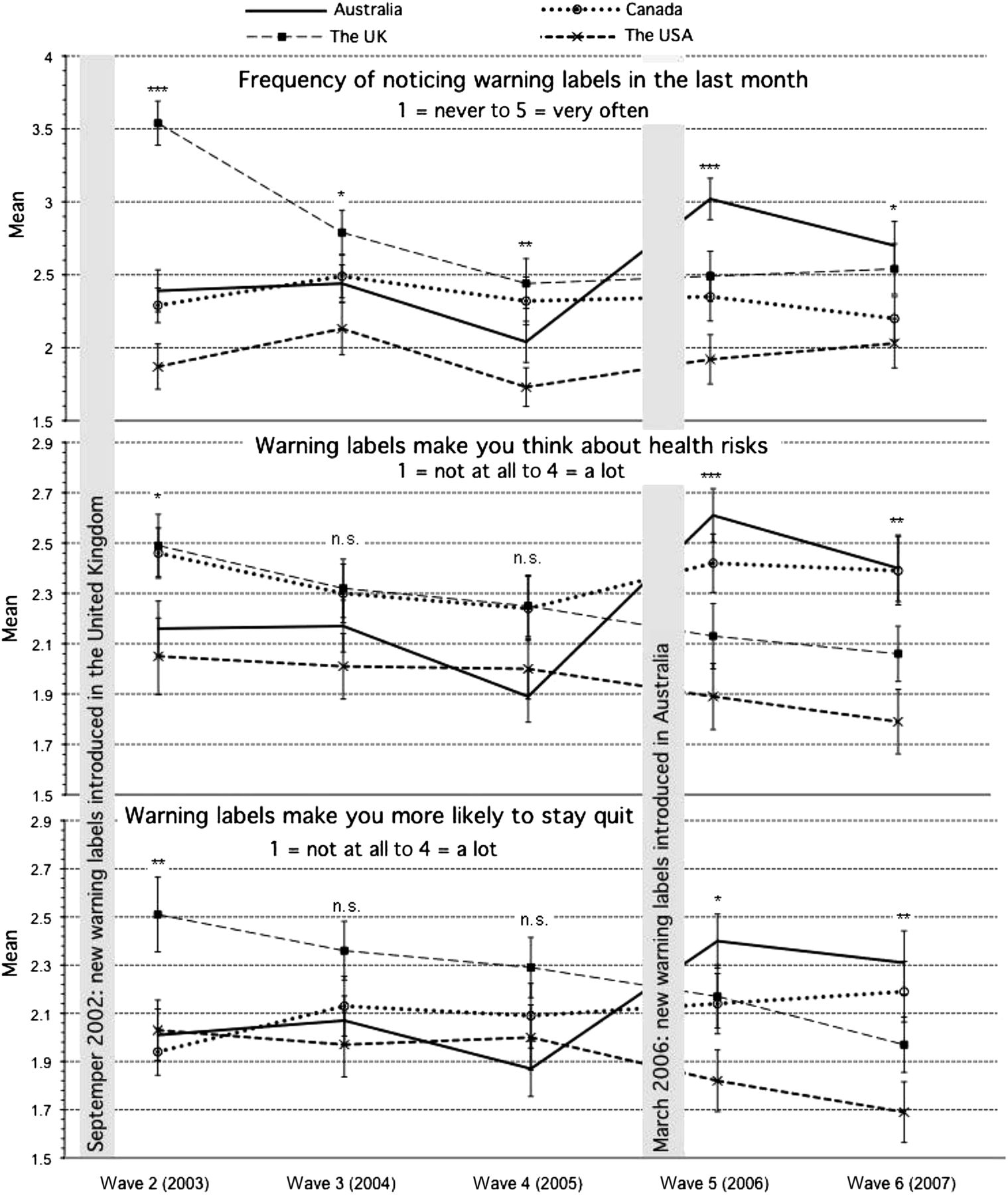
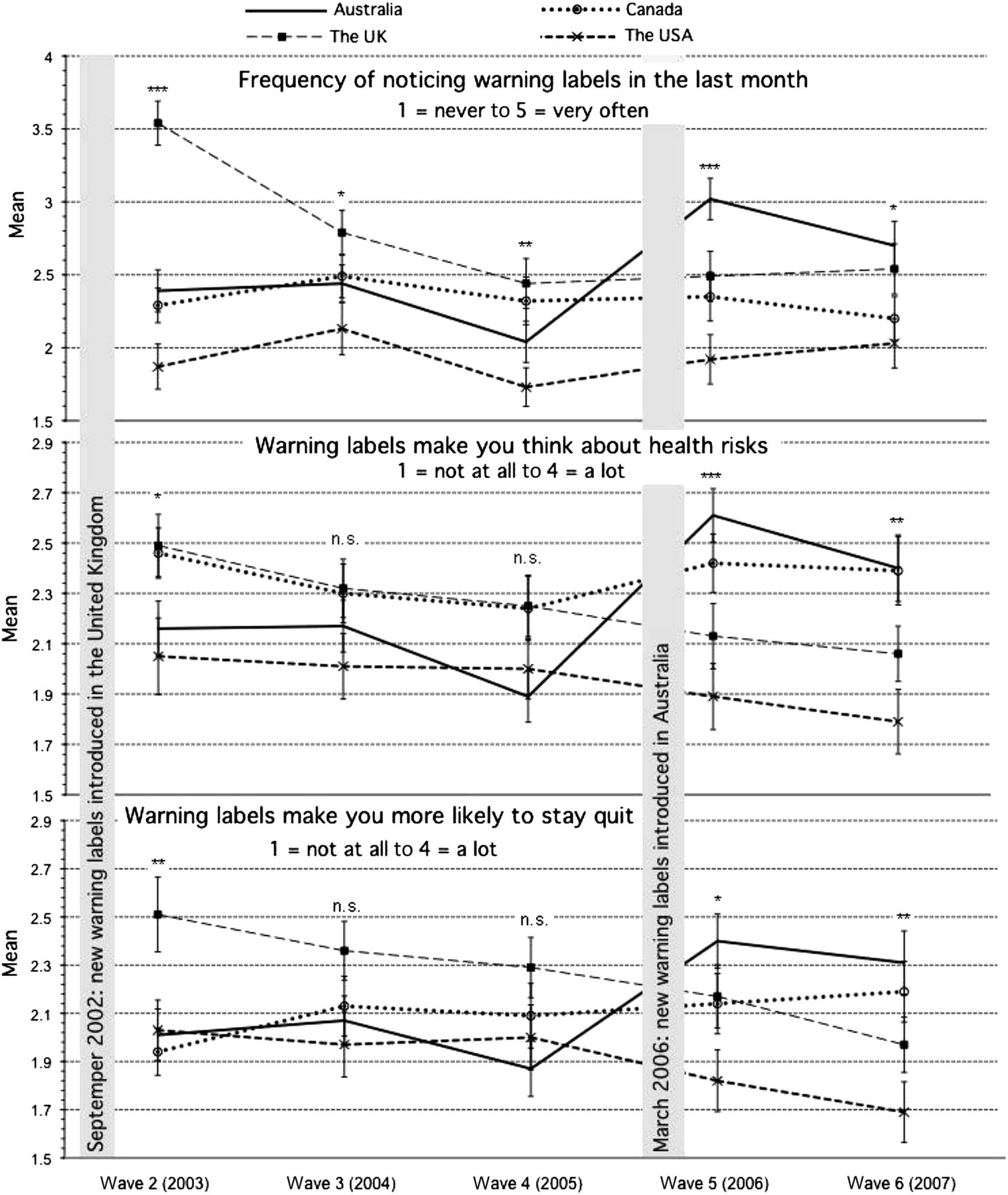
Country made no significant contributions to directly predicting relapse in any of the models we tested; however, there were some significant variations by country in the responses to the WL variables themselves, measured at quit baseline. Figure 2 shows that country differences were possibly related to label size and features. The US warnings received generally low ratings, whereas the Canadian warnings received generally higher ratings. Figure 2 also indicates peaks in the UK and Australian ratings in the survey waves (2 and 5, respectively) immediately following the introduction of new labels.
{kind=link}
{kind=link}
Mean levels of reporting for warning label variables by country and wave, among participants quit at that wave (the baseline quit wave). Error bars represent 95% CIs. *p<0.05, **p<0.01, ***p<0.001, n.s. = not significant: results of global analyses of variance for country differences at each wave (see text for more details).
We now turn to a consideration of the factors affecting the levels of reporting WLs make you more likely to stay quit. A mixed 4 (country) × 5 (quit baseline survey wave) analysis of variance indicated that responses to this variable differed significantly by country, F(3, 1890)=6.1, p<0.001, and there was also a significant country × survey wave interaction, F(12, 1890)=2.6, p<0.005 (see lowest panel of figure 2). As country and survey wave were entangled with label novelty, size and type in our data, we attempted to clarify the factors responsible for the country differences by creating three dummy variables relating to these WL qualities at participants' quit baseline wave. Novelty was the time in years (square root transformed) since the introduction of a new WL; size (small or large) contrasted the small US labels with the larger ones in the other three countries and type differentiated text from graphic labels. However, the nature of the data meant that novelty could not be completely structurally separated from either size or type, with more recent warnings also always being either larger, graphic or both. We conducted three binary logistic regressions predicting the bivariate associations (controlling for baseline quit length) of label novelty, size and type with reporting that WLs make you ‘a lot’ more likely to stay quit (vs the other three categories combined). These indicated novelty (OR=1.26, 95% CI 1.15 to 1.38, p<0.001) and size (OR=1.56, 95% CI 1.14 to 2.13, p<0.01) were positively associated with reporting that WLs make you ‘a lot’ more likely to stay quit, but there was no significant effect of type (p>0.05). Given the collinearity, an analysis containing all three was not meaningfully interpretable, beyond the finding that novelty had the strongest relationship with the outcome. However, label novelty, size and type did not directly predict relapse when included in our main regression analyses (not shown).
Discussion
Our results provide the first prospective evidence that WLs can have a protective benefit for recent ex-smokers over a period of at least 1 year after quitting. Our findings translate to a relapse rate over the next year of around 41% among ex-smokers who said that warning labels make them ‘a lot’ more likely to stay quit compared with 50% among those reporting that WLs make them ‘not at all’ more likely to stay quit. This result remained robust to the effects of exposure to tobacco, urges to smoke, self-efficacy to stay quit and prior level of addiction while smoking. Given that self-efficacy and frequency of urges have been shown to mediate the effects of most other possible determinants of relapse,17 ,28 this is a notable reduction in relapse. Furthermore, this result cannot be attributed to a subgroup of recent quitters who are finding it particularly easy to stay quit, as excluding those participants who reported never noticing WLs (a proxy for reduced cigarette salience and/ or exposure) actually increased the effect size. We do not know whether the effect remains consistent as a function of time quit. In addition, our sample under-represents early relapsers, so we do not know if the effect is the same for early as for later relapse. It should also be noted that, largely because of this under-representation, our study greatly underestimates total relapse.
As expected, this study confirmed that exposure to cigarettes and cigarette-related cues post-quitting is associated with a greater likelihood of relapse. However, this relationship can be eliminated by controlling for other measures that relate to the presence of smoking-related cues in the environment (such as friends smoking and frequency of urges to smoke) or by excluding those who report never noticing warnings at all. The pattern of results suggests that noticing the cigarettes themselves might only be a risk factor when it leads ex-smokers to think about smoking, but if they use the warning to actively resist, this strategy is protective.
Some caution should be exercised in concluding that the associations found here are causal. This was not a controlled experiment and it is possible that those who report using the WLs are a group who were just more motivated to quit. However, as health concerns and other measures of motivation are typically not associated, or negatively associated with relapse,25 and the effects are robust to controlling for the main known predictors, we think this unlikely. Furthermore, the prospective study design means that the experience of the outcomes cannot be a cause of the effects found, as can occur with cross-sectional designs. We acknowledge that some may wonder how WLs could act to prevent relapse when a recent review29 concluded there is no evidence for effective relapse prevention from dedicated interventions. However, unlike these interventions, which need to act beyond the period when they are being implemented, WLs are typically available for use at moments of relapse crisis.
It is notable that those lost to follow-up were both more likely to react to health warnings and to be embedded in a more smoking-related environment. Data from the ITC study show that ex-smokers are more likely to drop out30 and anecdotally some contacted report this is because now they have quit they do not want to think about smoking again. This suggests that dropouts may be prone to use avoidance as one of their relapse prevention strategies. We see no reason why the retention of this group would eliminate the effects we found, especially as systematically eliminating those not noticing warnings increased effect size. Arguably, given participants lost to follow-up are more likely to be ex-smokers and they were also more likely to report that WLs make them ‘a lot’ more likely to stay quit, our findings would be expected to be even stronger had they been retained in the cohort.
Our findings come from recent quitters from high-income countries, which have been among the strongest in educating the public about the harms of smoking. However, given that health warnings seem to have at least as strong an effect on smokers in less affluent countries and those with shorter histories of tobacco control efforts,2 we see no good reason why the results would not generalise.
WL properties (novelty, size and text vs graphic) did not directly predict relapse but appear to have an indirect effect through affecting the likelihood of the warnings being seen as very protective. Our results indicated that novelty was relatively more important for increasing reactions to WLs, and label novelty is likely to underlie the country differences we found. However, our measure of novelty contains an element of stronger warnings, as all newer warnings were larger and/ or graphic, so we cannot conclude that this is entirely a recency effect.
We theorise that the mechanism by which WLs help ex-smokers to stay quit involves some sort of active use of the warnings, for example, to help generate reasons for resisting temptations to relapse, and is not something that occurs automatically. Mere noticing of the labels was associated with increased relapse, and a protective effect was not found among those reporting that the labels simply made them think more about the harms associated with smoking. We therefore speculate that the individuals who report that WLs will help them a lot to stay quit have (consciously or not) devised strategies to use them to do exactly that. Relapse to smoking is theorised to occur at moments when the balance of motivational forces supporting quit maintenance are weaker than the motives for smoking.31 Pack warnings are likely to be present at moments of relapse risk, and when they are attended to, even weak effects on motivation could tip the balance in favour of maintaining abstinence on any given occasion, multiplying over numerous crises and thereby producing marked effects on relapse rates. It would be interesting to test this idea by actually encouraging recent quitters to use this strategy and see if it reduced relapse. Our findings suggest that this might only need to be focused on those reporting some more than minimal exposure to packs. Given no likely downside of encouraging use of WLs to prevent relapse and a possible large upside, we recommend that health professionals encourage all quitters to consider pack warnings as a potential tool to help counter their urges to resume smoking.
Despite the documented effectiveness of WLs, a recent review indicated that many FCTC signatory countries, particularly those with lower incomes, are failing to meet FCTC standards.32 These are sometimes the countries where less resources are devoted to tobacco control and raising public awareness of the risks of smoking. The implementation of WLs poses very little cost to government. This study provides more evidence that prominent WLs on cigarette packets should be a priority for parties to WHO FCTC33 and indeed for all countries wanting to reduce smoking prevalence.
What is already known on this subject
-
WLs are an important source of information for smokers and also for non-smokers.
-
Experimental smokers and non-smokers report that WLs help to discourage them from smoking.
-
Health WLs on cigarette packets have been shown to increase interest in quitting and quitting activity among smokers.
What this study adds
-
This is the first study to show that WLs can inhibit relapse. Recent quitters who reported that WLs help them a lot to stay quit were less likely to relapse in the following year compared with those who reported that WLs would not at all help them to stay quit.
Acknowledgments
We would also like to thank members of the Data Management Core at the University of Waterloo for assistance in preparing the data for this analysis.
References
Footnotes
-
Funding The ITC Four-Country Survey is supported by multiple grants including R01 CA 100362 and P50 CA111236 (Roswell Park Transdisciplinary Tobacco Use Research Center) and also in part from grant P01 CA138389 (Roswell Park Cancer Institute, Buffalo, New York), all funded by the National Cancer Institute of the United States, Robert Wood Johnson Foundation (045734), Canadian Institutes of Health Research (57897, 79551), National Health and Medical Research Council of Australia (265903, 450110, APP1005922), Cancer Research UK (C312/A3726), Canadian Tobacco Control Research Initiative (014578); Centre for Behavioural Research and Program Evaluation, National Cancer Institute of Canada/Canadian Cancer Society. The funding agencies had no role in the study design; collection, analysis or interpretation of data; writing of the manuscript or the decision to submit the manuscript for publication.
-
Competing interests None.
-
Patient consent Participant consent was obtained verbally during the telephone interview process.
-
Ethics approval All waves of the study have received ethical approval from the relevant institutional review or research ethics committees at The Cancer Council Victoria (Australia), Roswell Park Cancer Institute (USA), University of Waterloo (Canada) and University of Strathclyde (UK).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
↵i In October 2008, after the present data collection period, the UK implemented graphic health warnings covering 43% of the front and 53% of the back of cigarette packets.
-
↵ii The USA has recently passed legislation to require graphic warnings to cover 50% of the front and back of cigarette packs, which are expected to be in effect by October 2012, in compliance with FCTC standards, although current legal action may change this. Australia is also increasing the size of its warning and requiring standardised or plain packaging of tobacco products, with legislation to be fully in effect by December 2012.
-
↵iii Additional details of these analyses may be obtained on request from the corresponding author.