Article Text

Abstract
OBJECTIVES To investigate the relation between lung function in employees and exposure to environmental tobacco smoke (ETS) at work and elsewhere.
METHODS Never smokers in employment (301) were identified from the fourth Scottish MONICA survey. They completed a self administered health record, which included details of exposure to ETS, and attended a survey clinic for physical and lung function measurements, and for venepuncture for estimation of serum cotinine. Differences in lung function in groups exposed to ETS were tested by analysis of variance (ANOVA), the exposure-response relation by a linear regression model, and a case-control analysis undertaken with a logistic regression model.
RESULTS Both men and women showed effects on forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC) from exposure to ETS—higher exposure going with poorer lung function. This was found at work, and in total exposure estimated from ETS at work, at home, and at other places. Linear regression showed an exposure-response relation, significant for ETS at work, total exposure, and exposure time/day, but not at home or elsewhere. Compared with those not exposed to ETS at work, those who were exposed a lot had a 254 ml (95% confidence interval (95% CI) 84 to 420) reduction in FEV1, and a 273 ml (60 to 480) reduction in FVC after adjusting for confounders. Although lung function was not significantly associated with serum cotinine in all the data, a significant inverse relation between cotinine concentration and FVC occurred in men who had had blood collected in the morning. Case-control analysis also showed a significant exposure-response relation between ETS, mainly at work, and lung function. A higher exposure measured both by self report and serum cotinine went with lower lung function.
CONCLUSION The exposure-response relation shows a reduction in pulmonary function of workers associated with passive smoking, mainly at work. These findings endorse current policies of strictly limiting smoking in shared areas, particularly working environments.
- passive smoking
- working environments
- lung function
Statistics from Altmetric.com
Passive smoking is exposure of a person to environmental tobacco smoke (ETS) resulting from another person smoking. It can occur at the workplace, at home, and in public areas, where there is active smoking. Passive smoking includes both expired and sidestream smoke, and contains many of the same carcinogenic and toxic agents as mainstream smoke inhaled by active smokers. This may produce effects similar to those associated with active smoking. The adverse health effects of active smoking have been unambiguously shown in adults as well as during young adulthood,1 2 and passive smoking has also been shown to increase risk of cancer and cardiovascular disease.3 4 However, the reported effects of ETS on adult pulmonary function are inconsistent or less conclusive,5-21 although passive smoking significantly reduced lung function in children.22-24 Adult pulmonary function may be affected by many other factors over a lifetime. Some previous studies failed to include potentially important epidemiological variables and to adjust for potential confounding factors, and inclusion of subjects with different backgrounds might reduce the power to detect the effects of ETS on lung function. There was also a possibility of bias in reporting smoking habits, which may have resulted in active smokers being classified as passive only. Most previous studies of exposure to ETS have dichotomised exposure into unexposed and exposed categories, which may be crude for assessment of exposure and might lead to a bias (misclassification) because such exposure may vary over time. Furthermore, there was no exposure-response relation in most of the previous studies, which could be an obstacle to assuming a causal association between exposure to ETS and reduced lung function in adults. In this study, we carried out an analysis within the fourth Scottish MONICA survey on men and women in current full time employment to investigate whether the reduction of lung function in adults was significantly associated with exposure to ETS, whether there was a significant exposure-response relation, and where the exposure was occurring.
Subjects and methods
Subjects were derived from the fourth Scottish MONICA survey in 1995, which followed a similar procedure to the Scottish Heart Health Study.25 Adults aged 25–64 years were randomly selected from general practitioner lists in north Glasgow, Scotland. The sample was stratified by sex and 10 year age bands to obtain similar numbers of participants of each age. In total, 1836 subjects (865 men, 971 women) participated in the fourth Scottish MONICA survey, with a 65.8% response rate. They completed a self administered personal health record and a food frequency questionnaire. Details of active and passive smoking were recorded. Current smokers were defined as those who responded to the question, “Do you smoke cigarettes now?”—Yes, regularly or occasionally. Former smokers were those who responded negatively to this question but positively to the question “Did you ever smoke cigarettes?” Never smokers gave negative answers to both of these questions and smoked neither a cigar nor a pipe. To ascertain passive smoking, the subjects were asked “Are you regularly exposed to tobacco smoke from other people?” Responses gave four choices: yes, a lot; yes, some; yes, a little; or no, none at all. Three sources of exposure of ETS were given; workplace, home, and other places. A question for time of exposure to ETS was added: “On average, for how many hours a day are you exposed to other people's tobacco smoke?” Completeness was checked by a survey nurse.
Height and weight of the subjects were measured by standard techniques: height without shoes by portable stadiometer (Holtain, Crymych, United Kingdom) to the nearest 0.5 cm; weight without outer heavy clothing by digital scales (Seca, Germany) to the nearest 100 g. The forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC) were measured with a Microblab 3300 electronic spirometer (Micro Medical, England). Standardised field measurement procedures were used with subjects seated, without the use of nose clips. The study nurse demonstrated the technique, emphasising the tight fit between lips and tube and providing encouragement to breathe out as long and hard as possible to each subject. After one trial run, the best of three technically satisfactory manoeuvres was recorded by the machine. A blood sample was taken for cotinine (a metabolite of nicotine25 26) and other analyses. Socioeconomic deprivation was estimated by Carstairs scores based on census data on male unemployment, overcrowding, car ownership, and proportion of social classes IV and V in their postcode sector of residence.27
Based on the personal health record 602 subjects were identified as never smokers, and of them 301 (153 men, 148 women) who were currently in full time employment were selected for analysis. The reasons for such selection were that these subjects could provide full information on ETS including exposure at work, and would have less variation in other factors affecting lung function, being fit enough to work. Data were analysed with the SPSS statistical package (Windows version 9.0). Based on the questionnaire, the degrees of exposure to ETS were scored as: none at all=1, a little= 2, some=3, and a lot=4. Exposures to ETS at work, at home, and at other places were analysed separately, and then altogether. The total was obtained by adding up the three exposures; at work, at home, and at other places—the minimum score was 3 for non-exposure and the maximum was 12. Subjects with scores of 3 or 4 were defined as lowest, scores of 5–6 as a little, 7–8 scores as some, and 9–12 scores as highest exposure. Difference in lung function (crude and residuals, which were obtained from measured lung function minus lung function predicted from their age and height) between groups exposed to ETS were tested with ANOVA for men and women. Exposure-response relations were examined with a linear regression model for data on the groups exposed to ETS, exposure time/day, and serum cotinine concentrations. With a logistic regression model, a case-control analysis of those with residuals less than 0 versus those greater than 0 was carried out to further explore effects of exposure to ETS on lung function. Regression models were adjusted for (1) sex, age, and height where necessary, and further for (2) deprivation score and total energy intake, and finally adding for (3) respiratory symptoms including cough and phlegm to reduce possible confounding effects.
Results
Of 301 subjects, 150 men and 147 women had their lung function measured. Among them, one man and one woman had serum cotinine concentrations ⩾17.50 ng/ml (their values were 27.76 and 416.84 ng/ml respectively) and were excluded from the analysis due to possible deception about smoking in their questionnaire responses.26 Table 1 showed that there were differences in lung function among groups exposed to ETS for both men and women. These with some or a lot of exposure had a lower FEV1 and FVC than those with none or little exposure, although ANOVA showed that they did not reach the conventional significance level of p<0.05, perhaps because of the few subjects at the highest level of exposure. Men with higher exposure at work were younger and taller, whereas the reverse was found in women (table 1).
Age, height, and lung function in never smoking employees with different exposures to environmental tobacco smoke
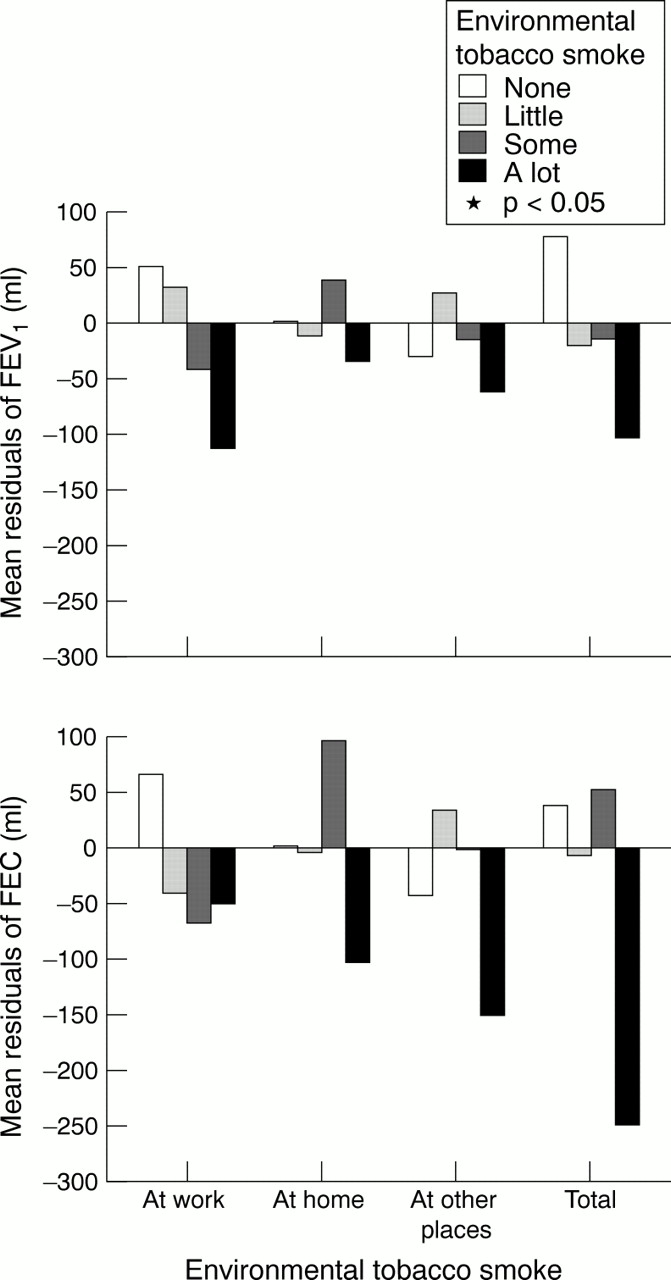
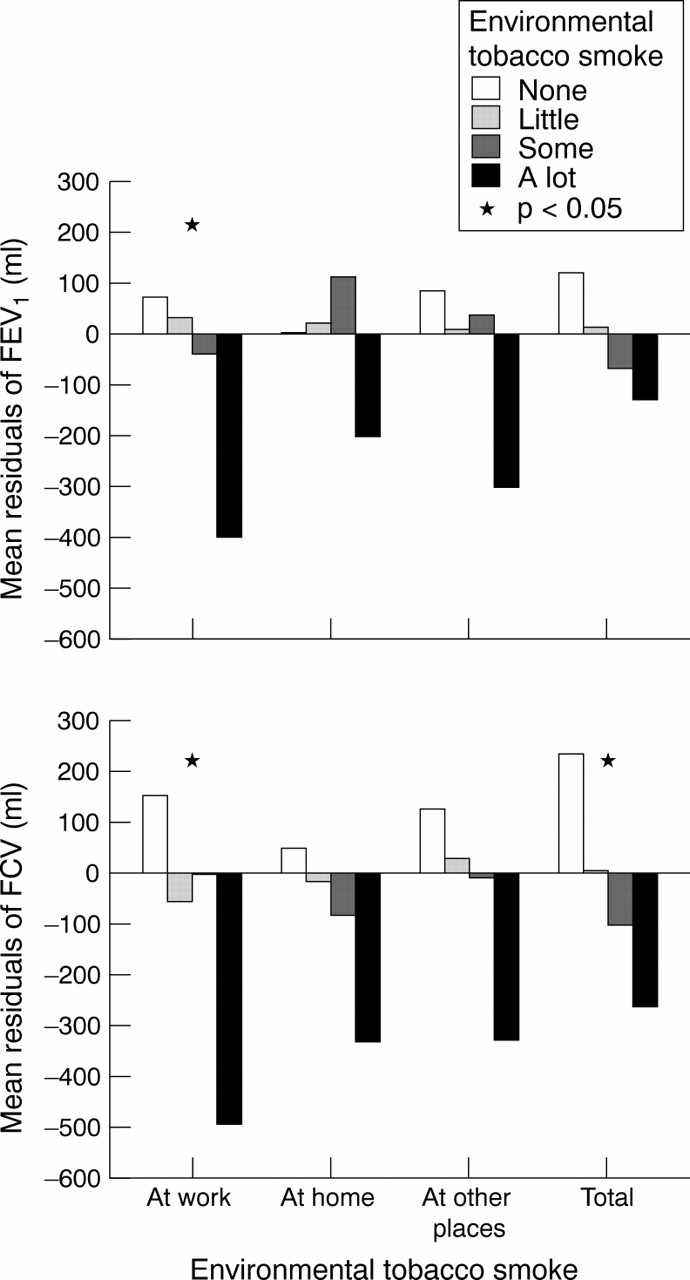
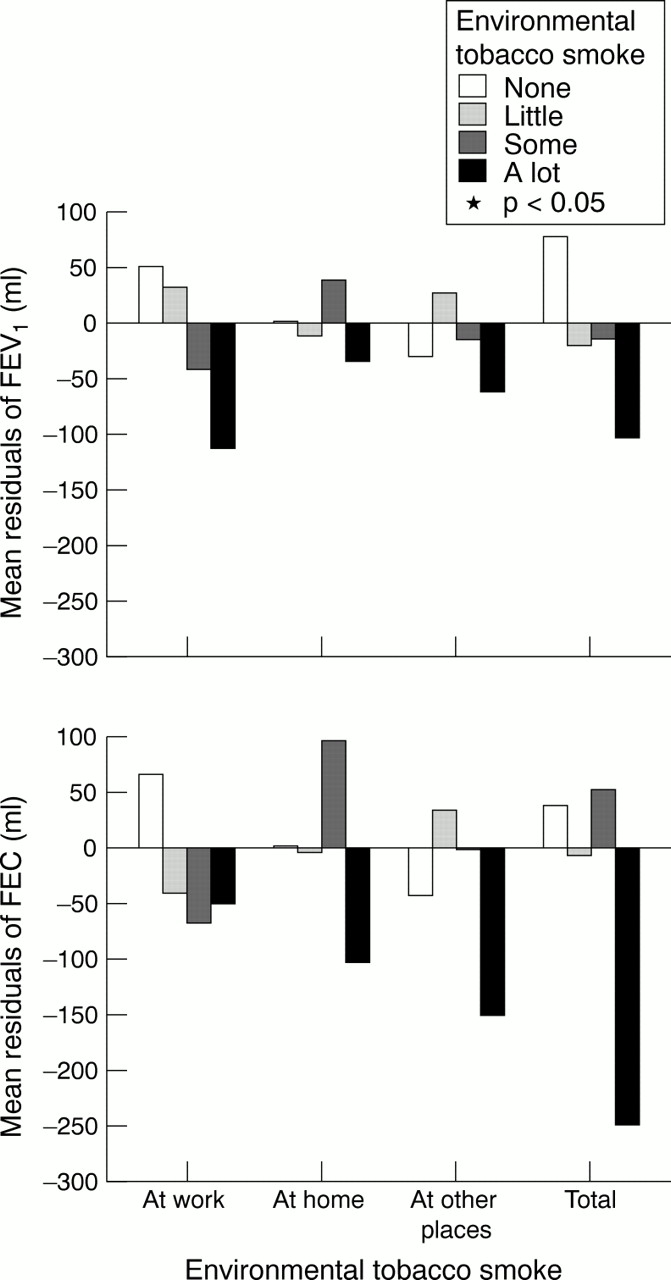
Figures 1 and 2 show the residuals of lung function with exposure to ETS. The predicted lung functions were:

Mean residuals of FEV1 and FVC by exposure to tobacco smoke for men.
{kind=link}
{kind=link}
Mean residuals of FEV1 and FVC by exposure to tobacco smoke for women.
in men FEV1=4.413×height−0.01374×age−3.355, FVC=5.667×height−0.008639×age−5.209;
in women FEV1=3.142×height−0.02531×age−1.328, FVC=4.031×height−0.02547×age−2.402.
For men there was a significant difference in both FEV1 and FVC between exposure to ETS at work, and possibly the total exposure to ETS (fig1), and for women results were similar but not significant (fig2).
Linear regression of the combined data for men and women showed that self reported exposure to ETS was negatively related to lung function (table 2). Significant results were found for exposure at work, for the total exposure, and for exposure time/day, but not for exposure at home or other places. Compared with those not exposed to ETS at work, those who were exposed a lot had a significant 254 ml (95% CI 84 to 420) reduction in FEV1, and a 273 ml (95% CI 60 to 480) reduction in FVC; and 1 extra hour of exposure to ETS per day was significantly associated with a 31 ml (95% CI 11 to 50) reduction in FEV1 and a 28 ml (95% CI 2 to 53) reduction in FVC after adjusting for confounders. Serum cotinine concentrations were not significantly related to lung function (table 2). In a separate data analysis for blood samples collected between 0700 and 1259 (morning) and between 1300–1700 (afternoon), however, there was a significantly inverse relation between cotinine concentrations and FVC for men with morning collection (n=72, β=−0.137, −0.126, and −0.125 after adjustments 1, 2, and 3 respectively, all p<0.05, table 2), but no significant relations were found for other groups (data not shown).
Linear regression of exposure to environmental tobacco smoke and lung function in never smoking employees
The case-control analysis showed that odds ratios (ORs) of reduced lung function significantly increased with self reported exposure to ETS at work and possibly with total exposure (table 3), but the increased ORs were not significant for exposure at home and at other places. In the combination of self reported exposure and serum cotinine concentrations (table 4), there was a significant difference in residuals of both FEV1 and FVC among groups exposed to ETS (ANOVA, both p<0.05), and the ORs of reduced lung function significantly increased with exposure.
Odds ratios of exposures to environmental tobacco smoke for subjects with low versus high lung function
Lung function with exposure to environmental tobacco smoke measured from a combination of questionnaire and serum cotinine
Discussion
The data from the fourth Scottish MONICA survey are well suited to assess the association between ETS and pulmonary function because the data are highly standardised. These include extensive information on passive smoking from three sources, at four levels of exposure and times of day, plus serum cotinine measurements. With serum cotinine concentration ⩾17.50 ng/ml as a cut off point, we were able to exclude two false non-smokers. The selection of the full time employees for analysis made the study more homogeneous. With socioecomonic deprivation (scores) as one adjustment, it was possible to rule out other confounding effects on reduction of lung function—for example, from living conditions and nutritent intake28-30—and a further adjustment for the respiratory symptoms might reduce possible biases of overestimation or underestimation of exposure from people with symptoms. All these adjusted analyses have shown consistent results and suggest that reduced lung function in employees was significantly associated with passive smoking; the effect was dose dependent and mainly from exposure to ETS at work.
Passive smoking has been significantly associated with some diseases.3 4 The evidence of an association between exposure to parental smoking and ventilatory impairment is relatively strong in children,22-24 but the findings of studies on the effects of exposure to ETS on lung function in adults are inconsistent. The disparate results of the previous studies could be explained by some other factors. Kauffmann et al 20 compared 3855 French women with 2200 American women in a study of the effects of passive smoking at home on lung function, applying similar methods of analysis in women from the French air pollution study and the United States six cities study. They found that there were adverse effects in French women older than 40 years of age, although no significant effect was found among the American women. This might be from differences in lifestyle and in housing conditions between Europe and North America, leading to differences in the actual levels of exposure to ETS. It is possible that the studies indicating a non-significant relation between exposure to ETS and lung function have involved lower exposures than experienced by our study population in which we measured four levels of exposure. In some studies with negative findings, most being from America, ventilation of the buildings may be much greater because of climate so that passive exposure to smoke is actually low.20 Within Europe, housing conditions in Britain would be expected to be more equivalent to those in France, and therefore it is not surprising for us to find a reduction of lung function associated with exposure to ETS.
Svendsen et al 8 noted that men with wives who smoked had lower pulmonary function than those with wives who did not smoke (FEV1 3.49 lv 3.59 l, p=0.04). They found no dose-response relation: for measurement at baseline, FEV1was 3.55 l in men with wives who smoked ⩾20 cigarettes/day, 3.41 l at 1–19 cigarettes/day, and 3.59 l with non-smokers. Results averaged over several visits were: 3.49 l, 3.26 l, and 3.49 l respectively. However, in this study we identified a significant exposure-response relation between self reported exposure to smoke and lung function among employees. If ETS is of causal importance in reduction of pulmonary function, the reduction of lung function should relate to the degree of exposure—that is, an exposure-response relation should exist. Our results are consistent with those in other studies,6 13 which report an exposure-response relation, and adds information on the exposure-response relation between passive smoking and reduction in lung function in adults.
When all data were analysed we did not find a significant relation between serum cotinine concentration and lung function. It might be explained by the following factors. Firstly, there could be an effect from missing data. In two men and 15 (over 10%) women serum cotinine measurements were not available, probably introducing a bias. We found a significant inverse association between cotinine concentration and lung function in men who had blood collected in the morning, whereas there was no such relation for women. A lower rate of missing cotinine data in men than women may partly explain this. Secondly, we considered that the cotinine was an indicator of recent exposure over 1–2 previous days due to a short half life and could be largely affected by the time since last exposure to passive smoking in view of its low concentrations. Benowitz31 suggests that cotinine concentrations resulting from exposure to ETS increase slowly, reaching a peak 4–6 hours after exposure. This assumes a steady state of exposure—this may be the case for the workplace and the home but exposure in our category, other places, may vary a lot. If the total exposure to ETS is variable, the time delay between exposure and blood sampling will have an effect. In the data of the Scottish Heart Health Study,26 we did not find a good correlation between self reported degree of exposure to ETS and cotinine concentration, and suggested that validity of different measures of exposure to tobacco smoke needed further investigation. We have carried out an analysis of data from all four Scottish MONICA surveys for the non-smokers in full time employment (data prepared for publication). The results showed that cotinine concentrations were more closely related to the self reported exposure to ETS within a defined time limit. Thus we considered that an effect from delay between exposure and the time of blood sampling could not be ruled out. Cotinine concentrations may not be a perfect gold standard in validating questionnaires on long term exposure to ETS.32 In view of this, we would suggest that both self reported exposure and serum cotinine are used to estimate the exposure. Such a combined measurement may be a better indicator of exposure to ETS.
Carey et al 14 reported that salivary cotinine predicted a reduction of lung function more than the self reported exposure. However, their estimation of exposure was dichotomised data, and only from exposure at the home. The authors explained that the finding may reflect the importance of exposure outside the home. Masjedi et al 12 also found that men exposed to ETS only at home had smaller (and non-significant) reductions in lung function than those exposed in the workplace. Our finding showed that among three sources of ETS, only exposure at work was significantly associated with reduced lung function. Compared with ETS at work, the total exposure to ETS showed a less clear exposure-response relation between ETS and reduced lung function (fig 1, fig 2, and table 3). This could be partly explained from the combining of data from the three sources of ETS, where the durations of exposure from each source were different.
The effects of ETS on pulmonary function in adults, if any exists, are more subtle than those of active smoking because the toxic agents in passive smoking are dilute compared with mainstream smoke in active smoking. For example, particulates are about 10 times lower in sidestream smoke than in mainstream smoke.33 A recent meta-analysis showed a 2.7% deficit in adult lung function resulting from exposure to ETS.14 Our data showed a greater effect of passive smoking than other studies.6 13 There are several possible reasons for this: (a) in this study four degrees of exposure to ETS were used to estimate the effect, (b) our subjects were more homogeneous than those in other studies and there was probably a healthy worker effect, (c) the subjects may be more sensitive to ETS in reduction of lung function as the Scottish people have lower estimated mean vitamin C intake than the other populations,34 and vitamin C could protect the lungs,19 30 and (d) more indoor ETS could be expected because in Britain most people spend most of their time inside buildings,28 housing conditions are more equivalent to France and are without the increased ventilation in America.20 We also found that compared with exposure at home and at other places, the relation between ETS at work and lung function was more significant and greater. An explanation for the greater effect of exposure at the workplace is that the subjects would be exposed for about 7 hours, whereas at other places the actual contact and exposure to cigarette smoke was shorter.12
Our study has shown a significant inverse association between exposure to passive smoking and pulmonary function in working adults, and that such an association could be dose dependent. This suggests that ETS may lead to a reduction in pulmonary function in adults. Passive smoking has been a public concern for a while, because it is a major indoor pollutant to which a substantial segment of the population is exposed.28 35 Our findings suggest that, as well as its effects on the smoker, smoking at work may contribute to deterioration of lung function in non-smoking workmates, further evidence for its control.
Acknowledgments
This work was funded by the Scottish Office and British Heart Foundation.
References
Linked Articles
- Correction