Article Text

Abstract
Background: It is believed that health risks associated with smokeless tobacco (ST) use are lower than those with cigarette smoking. A systematic review was therefore carried out to summarise these risks.
Methods: Several electronic databases were searched, supplemented by screening reference lists, smoking related websites, and contacting experts. Analytical observational studies of ST use (cohorts, case-control, cross sectional studies) with a sample size of ⩾500 were included if they reported on one or more of the following outcomes (all cause mortality, oral and pharyngeal cancers, other cancers, cardiovascular diseases, dental diseases, pregnancy outcomes, surgical outcomes). Data extraction covered control of confounding, selection of cases and controls, sample size, clear definitions and measurements of the health outcome, and ST use. Selection, extraction and quality assessments were carried out by one or two independent reviewers.
Results: A narrative review was carried out. Many of the studies lacked sufficient power to estimate precise risks, mainly due to the small number of ST users. Studies were often not designed to investigate ST use, and many also had major methodological limitations including poor control for cigarette smoking and imprecise measurements of exposure. Studies in India showed a substantial risk of oral or oropharyngeal cancers associated with chewing betel quid and tobacco. Studies from other regions and of other cancer types were not consistent. Few studies have adequately considered the non-cancer health effects of ST use.
Conclusions: Chewing betel quid and tobacco is associated with a substantial risk of oral cancers in India. Most recent studies from the US and Scandinavia are not statistically significant, but moderate positive associations cannot be ruled out due to lack of power. Further rigorous studies with adequate sample sizes are required, especially for cardiovascular disease.
- smokeless tobacco
- systematic review
- epidemiology
Statistics from Altmetric.com
Smokeless tobacco (ST) is tobacco consumed orally, not smoked. It has been in use for as long as other forms of tobacco consumption and its use has increased.1 The main types of ST in Western countries are chewing tobacco and oral snuff. Chewing tobacco is predominantly used in the USA and snuff (snus) in Sweden. In developing countries, tobacco is mostly chewed with other ingredients. Chewing is practised in different ways: the main ingredients are usually areca nut (betel), betel leaf, lime and tobacco. Other types exist worldwide.2,3
Major reviews in the mid 1980s concluded that ST use has substantial negative health implications. A US Surgeon General report in 1986 concluded that “the use of snuff can cause cancer in humans” and “the excess risk of cancer of the cheek and gum may reach nearly 50-fold among long term snuff users”.4 ST use can be addictive, leading to oral leukoplakias (oral mucosal lesions), gingival recession, and may play a contributory role in the development of cardiovascular disease, peripheral vascular disease, hypertension, peptic ulcers, and fetal morbidity and mortality”.4 An IARC monograph in 1984 similarly concluded that snuff use causes cancer.5 Nevertheless, the negative health effects of ST use have been questioned. ST is not homogeneous1; there are significant differences in composition and production. Levels of the most powerful carcinogens—tobacco-specific N-nitrosamines (TSNAs)—vary widely in different ST products6 and recent production trends may have reduced these levels.7,8
The ecological analyses available to date from Western countries have been inconclusive. Sweden has a low rate of oral and pharyngeal cancers despite high ST use. The US states with highest ST use (West Virginia) do not have high rates of oral cancers.9 In Asia, the majority of ST studies have been carried out in India where both the habits and the negative outcomes (mainly oral cancers) are most prevalent, and strong dose dependent associations have been found.10–13 Tobacco here is generally used with other substances such as areca nut and lime, which may themselves be associated with oral disease.14–16
Although reductions in cigarette smoking have been achieved in many developed countries, these falls have begun to level off.17 Further reductions may be difficult to attain,18 despite a myriad of effective cessation products. Success rates regarding long term smoking abstinence are disappointing, with less than 50% of smokers quitting permanently.19,20 Persuading resistant smokers to reduce21 or to switch to less harmful products22–24 could benefit public health.23,25 Tilashalski et al23 estimated that, if all US smokers switched to ST use, 12 000 cases of oral cancer would occur each year, representing only 5% of all tobacco smoking related lung cancers and 50% of the oral cancers now attributed to cigarette smoking.22,23 This is controversial as the precise health effects of ST use are uncertain and are not necessarily limited to oral cancers.26 The health benefits of switching to supposedly “less harmful” smoked tobacco forms (such as cigars, pipes, low yield or light cigarettes) have been disappointing.20,25 Others argue that the development of new improved smoking cessation pharmacotherapies is preferable.26
This review has been carried out in an attempt to quantify the major health effects associated with ST use and to critically appraise the studies performed. Significant numbers of new studies have been published since the major reviews of the mid 1980s and early 1990s, and types of ST have changed. Many literature reviews have been published, mostly confined to a single health effect such as oral cancer,27–29 cancer,30–32 or periodontal disease.33–35 None appears to be “systematic” in its approach and all lack a search strategy or inclusion criteria.
METHODS
The objectives of the review were to (1) identify and describe epidemiological studies; (2) provide narrative and tabular summaries of results; and (3) interpret results including the potential impact on the population.
Criteria for considering studies for review
Types of studies
Analytical epidemiological studies were reviewed, provided they included users of a form of ST and a group who used no tobacco products or smoked cigarettes only. Small studies (total sample size <500) were excluded as they may be subject to publication bias and are more likely to be published if they are “positive”,36,37 while larger studies are likely to be published regardless of their finding and may provide more power. Excluded studies are listed in the appropriate tables of excluded studies for each health outcome. All the studies meeting the inclusion criteria are described in detail in appendix 1 (available on the Thorax website, http://thoraxjnl.com/supplemental; other appendices are available from the authors on request).
Types of outcome measures
Studies reporting one or more of the following health outcomes were included: oral/pharyngeal cancers, other cancers, all cause mortality, vascular diseases, dental health, complications of pregnancy, and surgery. Ideally, outcomes should be clearly defined according to International Classification of Disease system (ICD). The author’s statement that the study considered one of these outcomes was accepted. Excluding studies with no clearly defined outcomes may bias against older studies. Studies reporting on one or more “intermediate” outcomes such as blood pressure or lipid levels,38,39 or oral lesions such as leukoplakia were excluded.
Search strategy for identification of primary studies
A comprehensive search strategy was developed which included electronic databases, websites, and contact with experts. A small number of non-English language studies were identified but were not included (see appendix 2).
Relevant studies were identified by searching several electronic databases from inception (appendix 3). Databases searched include Medline, Embase, CINAHL, and Dissertation Abstracts. Both key words and MeSH headings were used. Websites (WHO, ASH UK, ASH US, NIH, CDC) were also searched using the key term “smokeless tobacco”. Contact was sought from experts including those in the tobacco industry (appendix 4) and supplemented by cross checking reference lists of articles (appendix 5).
The form of electronic searching for the databases (Medline, Embase, CINAHL) was: (ST or synonyms) and (epidemiological studies or synonyms). The search strategy for study types was adapted from previous reviews.40,41 The strategy was piloted in Medline and cross checked against possible terms for ST use.42 We checked that the omission of brand names (such as Skoal, Hawken, etc) did not affect the number of potentially relevant hits.
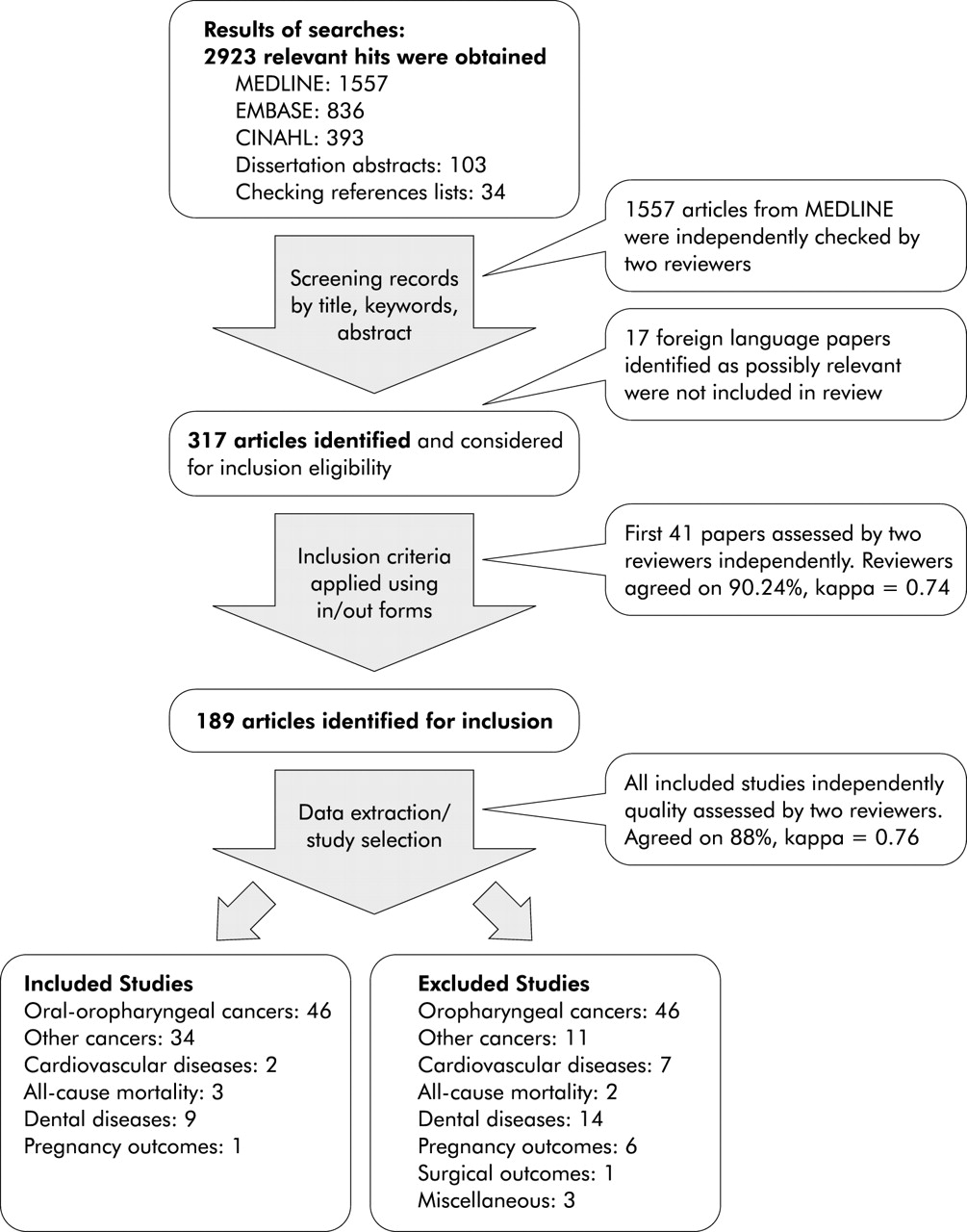
The electronic searches identified 2889 records and a further 34 were obtained from checking references, giving a total of 2923 relevant hits although these included some duplicates. The websites also obtained many “hits” (appendix 4).
The downloaded records were imported to Reference Manager and the titles, keywords, and abstracts were scanned by at least one reviewer. A conservative approach was used—that is, all records were checked unless sufficient details were available to decide that the study was definitely not relevant. The first 1557 articles downloaded (from Medline) were also screened independently by a second reviewer. Articles identified in this way (n=317) were scrutinised and/or a copy obtained to consider eligibility further. A total of 189 possibly relevant articles were identified. Ideally, two reviewers should independently assess each study for inclusion and extract data. The first 41 papers assessed for inclusion by the co-reviewer were independently considered by the first reviewer. Agreement was good (90.2%, kappa=0.74), and disagreements were resolved by discussion (fig 1).

{kind=link}
Flow chart of search strategy for review of literature on smokeless tobacco.
An inclusion criteria form and data extraction form was developed41 (appendix 6) and pilot tested on four articles. Once initially identified, one of two reviewers extracted data from all the articles to be included.
Unlike randomised controlled trials, there are no generally accepted lists of appropriate quality criteria for observational studies.43,44 Rather than using scoring methods, specific aspects of quality such as control of confounding, selection of cases and controls, sample size, clear definitions of the outcome of interest and ST use, evidence of a dose-response relationship between ST use and outcomes are described for each study. Both reviewers independently classified each study as either methodologically adequate or flawed (coded as A or F under “Comments”, appendix 1). Agreement was high (kappa=0.76). Flawed studies were those which either (1) contained <10 cases among ST users, or (2) did not control for the most “critical” confounders (age, sex, and use of other tobacco products), or (3) did not state what form of ST was used or did not perform separate analyses for each type of ST.
All studies meeting the inclusion criteria are listed in appendix 1, but only those achieving these quality criteria and published after 1980 are described in this paper. These are cross referenced to the tables in appendix 1 (ID number).
RESULTS
Studies excluded are listed alphabetically by first author under the categories of “oral and oropharyngeal cancers”, “other cancers”, “cardiovascular diseases”, “all-cause mortality”, “dental diseases”, “pregnancy outcomes”, “surgical outcomes”, and “miscellaneous” (appendix 7).
The results for each study included in the review are presented in a series of tables (appendix 1). The health outcomes are listed in the same order as above. Separate tables are prepared by region (US, Scandinavia, Asia, other) for each outcome and are then listed by study type (cohort study, case-control study, cross-sectional study). Within these subsections the studies are listed in date order.
Oral and pharyngeal cancers
US case-control studies
One study from a Veterans Hospital in New Jersey found no increased risk of oral cancer among users of either snuff or chewing tobacco, and no trend in risk according to the duration of chewing (ID8).45 This study included many ST users although it was mainly concerned with smoking and alcohol consumption. Sites included were not clearly defined and the case series was incomplete. Although important confounders were analysed, the reference categories for both tobacco smoking and alcohol consumption were “minimal users”, including smokers of 1–5 cigarettes per day. This is likely to underestimate the risk associated with ST use.
Another large population based study using cancer registry data in Florida found a strong association between ST use and cancers of the mouth and gum (for example, odds ratio (OR) 11.2, 95% CI 4.1 to 30.7), salivary glands, and larynx. This study was unable to control for use of alcohol (ID10) and the number of ST users was small.46
In the late 1970s a key study was carried out among women with oral and pharyngeal cancers in North Carolina which found strong associations with ST use (ID13).47 The OR for snuff dipping was 4.2 (95% CI 2.6 to 6.7) among white women for cancers of the gum and buccal mucosa. Significant dose-response relationships were observed—for example, an OR of 47.5 (95% CI 9.1 to 249.5) for those who had used snuff for 50 years or more. This study was well designed with clear definitions of the sites included, selection of controls, and important confounders considered. A high proportion of interviews were carried out with “next of kin” among cases (51%) compared with controls (21%). This study remains the strongest evidence for an association of ST use with oral cancers in the US, although it is limited to women and was carried out many years ago.
Scandinavian case-control studies
Swedish studies are easier to interpret than those in the US as only moist oral snuff is used. Scandinavian studies are also facilitated by the excellent population based statistical information available. However, there may be important differences between different snuff brands.
In south Sweden and Stockholm a recent study of men with oesophageal and oral cancers found a raised risk for ex-snuff users compared with never users of tobacco (ID19).48 The risks were higher for ex-users than for current users, suggesting possible selection bias. The OR for current users was 3.3 (95% CI 0.8 to 12.0) and for ex-users was 10.5 (95% CI 1.4 to 117.8). This study lacked power as the number of never users of tobacco was small. Control of confounding was mostly limited to age and region, and cases were interviewed in hospital while population based controls were interviewed at home, suggesting possible recall biases.
Similar results were found from an earlier study in northern Sweden of cancers of the oral cavity (ID20).49 The most common tumour was lip with an OR of 1.8 (95% CI 0.9 to 3.7) for ex-snuff users but close to unity for current users. This study is methodologically strong, with high response rates and clear definitions of sites included and snuff use. A large proportion of the cases had died, so responses were obtained from relatives. Furthermore, the number of snuff users was relatively small.
Asian studies
Asian studies are less equivocal in their interpretation than those from Scandinavia and the US. Both oral cancers and ST use are many times more prevalent, particularly in India. Some studies have been able to collect substantial trend data including frequency and years of use, and age at starting.11,50 However, the use of ST is different, with tobacco being chewed mainly with other ingredients which may be carcinogenic. The duration and amount used daily may also be higher, as traditionally Indians commence chewing when young and chew regularly, possibly to stave off hunger.51 These studies provide strong evidence that the oral use of tobacco can be carcinogenic.
Cancer registry data from Bhopal showed a sixfold increased risk for cancer of the oral cavity (OR 5.8, 95% CI 2.6 to 9.5) after adjusting for age and smoking (ID24).52 Chewing for over 30 years was associated with an OR of 23.9 (95% CI 12.0 to 47.3) for oral cancer. The attributable risk of cancer of the oral cavity for tobacco chewers was estimated at 84.4%. Outcomes were clearly defined in this study but the response rates were unclear and alcohol consumption was not controlled for. Information on ST use among cases was obtained from a separate survey in Bhopal which could bias risk estimates.
This is supported by two studies of men with tongue and oral cancer from Bombay (ID25, ID26).53,54 Statistically significant ORs were found for cancers of the anterior two thirds of the tongue after multivariate analysis (OR 1.7, 95% CI 1.2 to 2.6) and for the whole oral cavity combined (OR 2.6, 95% CI 2.1 to 3.4), but not for the posterior third of the tongue (OR 0.9, 95% CI 0.6 to 1.2). Trends for all oral cancers were found with increasing daily frequency of use and duration of use in years—for example, crude OR 1.3 (95% CI 0.9 to 1.8) for 1–10 years of use and 3.9 (95% CI 2.5 to 5.8) for 31+ years of use. This study was well designed with clear definitions of outcomes and good control of potential confounders.
Three further studies considering dose-response relationships for different cancer locations were carried out in Kerala, India in 1983–4 (ID28–30).11,12,55 These were methodologically sound and the sites included were clearly described. Control of confounding was good (alcohol consumption, duration of bidi smoking, snuff use).55 Strong significant associations and dose-response relationships were observed for cancers of the gingiva, tongue and floor of mouth, and oral cavity.12,55 For example, for cancers of the buccal and labial mucosa the OR for men associated with chewing ⩽10 times per day was 6.9 (95% CI 2.8 to 16.8), while those who chewed >41 times per day had an OR of 37.8 (95% CI 19.5 to 73.1), adjusted for age and religion.12
One prospective cohort study was carried out among villages in India (ID23).56 The sample size was large with frequent follow up, allowing for changes in tobacco habits over time. Oral cancer (and oral lesions) occurred almost solely among those who practised tobacco habits in some form, and was always preceded by some type of precancerous lesion.57 Indeed, malignant transformation of leukoplakia was not observed in those who smoked but did not chew tobacco; the rate of malignant transformation per 1000 persons per year was estimated as 9.7 in those who chewed, 5.0 in those with mixed tobacco habits, and zero in those who smoked only or had no habits (only six cases of leukoplakia had no tobacco habit).58 Despite the large sample size and fairly long follow up period (10 years), only 23 new cases of oral cancer were observed.
Other regions
Strong associations between “toombak” use and squamous cell carcinoma of the lip, buccal cavity, and floor of mouth were found in a case-control study in Sudan (ID41).59 The OR was 7.3 (95% CI 4.3 to 12.4) compared with hospital controls and 3.9 (95% CI 2.9 to 5.3) compared with population controls. The ORs for squamous cell carcinoma of the tongue, palate, and maxillary sinus were not statistically significant. All neoplasms were found at sites of preference for placement of toombak quid. Toombak is manufactured using a different tobacco species (N rustica) mixed with sodium bicarbonate. This study had clearly defined outcomes and reasonable control of confounding.
Other cancers
US case-control studies
A number of different cancer sites were identified including the urinary tract (bladder, kidney), stomach, and lung. Cigarette smoking was usually included as a variable but ST use was not the main focus of any of the studies, and most had few ST users.60–63 ST use was not usually clearly defined and no information on possible dose-response relationships was provided in any study. No significant association was found between ST use and cancer outcomes in most studies. Among studies meeting the quality threshold, no statistically significant relationship between ST use and bladder cancer was found (ID60).60 One estimated a raised OR of borderline significance for chewing tobacco and renal cell cancer among men (OR 4.0, 95% CI 1.1 to 14.2) (ID61).63
Scandinavian prospective cohort study
Cancer mortality was not significantly higher in snuff users in Sweden; relative risk (RR) 1.2 (95% CI 0.8 to 1.9) in subjects aged 35–54 years and 1.0 (95% CI 0.8 to 1.3) in those aged 55–65 years (ID85).64
Scandinavian case-control studies
Lagergren et al65 analysed patients with adenocarcinoma of the oesophagus or gastric cardia and oesophageal squamous cell carcinoma (ID70). Many potential confounders were considered including age, sex, education, cigarette smoking, alcohol consumption, dietary intakes of fruit and vegetables and energy intake, BMI, reflux symptoms, and physical activity. Snuff users had an OR of 1.2 (95% CI 0.7 to 2.0) for oesophageal adenocarcinoma compared with never users. No trends were found for years or intensity of use. The results were similar for those with adenocarcinoma of the gastric cardia (OR 1.2, 95% CI 0.8 to 1.8). For cases of oesophageal squamous cell carcinoma the adjusted OR was 1.4 (95% CI 0.9 to 2.3). Hansson et al66 found no statistically significant relationship and no dose-response trends for any of the three types of gastric cancer (ID71).
Asian case-control studies
Six studies considered other cancer outcomes. Unlike US studies, most of these had sufficient numbers of ST users among both cases and controls and were designed specifically to consider the association between cancer and ST use.67,68
Oesophageal cancer
One study from Assam (ID74) found raised OR for chewing tobacco associated with oesophageal cancer. This was consistent among users of different betel types, chewing tobacco alone, and in both men and women—for example, chewing tobacco alone was associated with an OR of 4.9 (95% CI 2.8 to 11.6) in men.69 Significant dose-response relationships were observed for all the variables considered (frequency of chewing per day, duration of chewing in years and starting age). The OR associated with chewing for >20 years was 10.6 (95% CI 5.6 to 17.3) in men and 7.2 (95% CI 2.6 to 14.2) in women, compared with 1.8 (95% CI 0.09 to 7.1) and 1.2 (95% CI 0.07 to 5.2) in men and women, respectively, who had chewed for <10 years.
Further studies of oesophageal cancer have been equivocal (ID76). In Bangalore, India70 similar risks were associated with chewing paan with tobacco (OR 2.9, 95% CI 1.5 to 5.4) and chewing paan only (OR 2.8, 95% CI 1.5 to 5.2) after multivariate analyses. The risk was highest for the lower third of the oesophagus (OR 6.6, 95% CI 2.1 to 21.2) and was not statistically significant for other parts of the oesophagus. The number of tobacco chewers was not high (79 cases, 96 controls) and some risks were imprecisely estimated. Although important confounders were considered, the response rates were low (62.5%). Another study from Kerala, India found no association between chewing betel and tobacco and oesophageal cancer (ID79).13
Larynx and lung
Little association was found between chewing betel and tobacco and cancer of the larynx (ID80)50 or the lung (ID75).52
Penile
In one study the adjusted OR for chewing tobacco was 4.0 (95% CI 2.7 to 6.1) and for snuff use the OR was 4.2 (95% CI 1.6 to 11.3) (ID 77).67 The OR of chewing tobacco use for <10 years was 1.7 (95% CI 0.9 to 3.3) compared with 3.6 (95% CI 2.5 to 5.3) for >10 years of use.
All cause mortality
Asian prospective cohort studies
The age adjusted RR of tobacco chewing for all cause mortality over a 10 year follow up period (reference group “no habit”) was 1.2 and 1.3 for men and women, respectively (statistically significant for women) (ID83).71 For those with mixed habits (smoking and pan together) the RR was statistically significant for men only (1.4 compared with 1.7 for women (CI not presented)). Similar results were found for other analyses from different parts of India (ID82, 84).56,72
Other
A prospective cohort study of cardiovascular disease mortality (ID85) estimated a RR of all cause mortality of 1.9 (95% CI 1.6 to 2.4) in those aged 35–54 years and 1.2 (95% CI 1.0 to 1.3) in those aged 55–65.64
Cardiovascular disease
Scandinavian prospective cohort study
A study of ST use and cardiovascular disease (CVD) was carried out in Swedish construction workers (n=135 036) (ID85).64 Snuff use was defined as current and exclusive use—that is, users were never smokers. Among those aged 35–54 years the RR for ischaemic heart disease (IHD) was 2.0 (95% CI 1.49 to 2.9), for stroke 1.9 (95% CI 0.6 to 5.7), and for all CVD deaths 2.1 (95% CI 1.5 to 2.9). However, the associations were smaller and not all were statistically significant in those aged 55–64 (IHD 1.2, 95% CI 1.0 to 1.5; stroke 1.2, 95% CI 0.7 to 1.8; CVD 1.1, 95% CI 1.0 to 1.4). This was explained as “a healthy worker effect”.
Scandinavian case-control studies
The MONICA (Monitoring Outcomes in Cardiovascular Disease) Sweden Project contributed two studies (ID86, 87),73,74 both of which found that snuff dippers had no increased risk of myocardial infarction (MI) compared with non-tobacco users. In the second study, more detailed information about ST (present use, previous use, amount, type of preparation, age of onset) was obtained from MI patients or next of kin. The OR for all and fatal MI remained non-significant after adjustments for various potential confounders.
Dental disease
Dental diseases are defined here to include both dental caries (tooth decay) and periodontal disease. Numerous studies have examined the relationship between cigarette smoking and dental diseases,28,33 but only a small number of cross sectional surveys of ST use and dental diseases have been undertaken.75 These are hard to interpret as the time relationship between ST use and dental disease is uncertain (previous exposure to ST use may be more relevant than exposure at the time of the study). Furthermore, many are in young people who may not have accumulated sufficient exposure to ST.
Dental caries
A recent analysis of adults from the NHANES (National Health and Examination Study) III study in the US suggested that chewing tobacco may be a risk factor in the development of root surface caries and possibly coronal caries (ID89).76 This large study used clearly defined caries indices, trained examiners, and found significantly raised ORs for decayed root surfaces among users of chewing tobacco (OR 3.24, 95% CI 2.0 to 4.4) compared with users of snuff, cigarettes only, cigars and pipes. Importantly, the decayed or filled root surfaces tended to match the side of the mouth on which the ST was used, although this did not reach statistical significance. Experimental evidence also suggests that chewing tobacco may be cariogenic due to its sugar content.77
A study among baseball players in Phoenix did not find any differences in dental caries between ST users and non-users, but the majority of ST users were snuff dippers (n=304) rather than users of chewing tobacco (n=89) (ID91).78 A further survey of adolescent boys in Atlanta (ID92) found a raised risk of caries in boys who used ST and also had gingivitis, significantly higher than in non-users without gingivitis (p<0.001).79
Higher levels of caries were observed in snuff dippers than in non-tobacco users among teenagers in Gothenburg (ID94).80 Controlling for cigarette smoking, a dose-response relationship was also shown between caries and the number of years of snuff use.
Periodontal diseases
Several US studies have examined the relationship between ST use and periodontal diseases. A study in Phoenix (ID91) was equivocal. No significant differences were found in gingival bleeding, pocket depth, or recession in at least one site of 12 teeth examined between ST users and non-users, but attachment loss of 4 mm or more was more common in snuff users both with (32.0%) and without (33.6%) oral lesions than in non-users (27.4%), p<0.05.78 A further study of adolescent boys in Atlanta (ID92) found associations between ST use and gingival recession, but not with gingivitis.79 The risk of gingival recession was only raised among ST users who also had gingivitis, but many important potential confounders such as diet and oral hygiene were not considered.
Adverse outcomes of pregnancy
Numerous studies have shown a strong association between cigarette smoking and adverse pregnancy outcomes, particularly low birth weight,81 but relatively few have considered the relationship of these variables with ST use.82,83 Generalisability of these studies elsewhere may be problematic, not simply because of differences in ST types but also in access to health care, nutritional status, cigarette smoking, and alcohol consumption.
The only study included in the review was of women in Delhi who delivered single infants in 1971–2 (ID98).82 The stillbirth rate was increased among tobacco chewers (crude OR 3.0, 1.3 to 6.7). Birth weights were presented for chewers and non-chewers by maternal weight, gestation, and social class. Overall, there was a reduction in birth weight of about 100–200 g in each stratum in chewers compared with non-chewers, and this was mainly attributed to the greater proportion of chewers who delivered at 36 weeks or earlier. Other potentially important confounders were not considered, although smoking was “rare” in this population.
Impact of ST use on the population
Most of the studies included in the review are hospital based case-control studies, so it is not possible to estimate the incidence rate and excess risk among ST users. From those studies which met the quality criteria, an estimate has been made of the population impact of ST use. The population attributable risk (PAR) is a measure of the proportion of the disease that could theoretically be prevented in the population if the use of ST was eradicated.
Table 1 estimates PAR fractions for oral cancers in each region and table 2 estimates PAR fractions for cardiovascular disease in Sweden. Where possible, PAR values for men and women were calculated separately. For other cancers it was considered that there were too few high quality studies. PARs are estimated using the formula:
Estimated number of deaths from oral cancer attributable to ST use in the US, Sweden, and India
Number of deaths from ischaemic heart disease (IHD) attributable to use of smokeless tobacco (ST) in Sweden
PAR = [prevalence × (relative risk – 1)]/[prevalence × (relative risk – 1)] + 1
It is assumed that the OR for each study is a reasonable estimate of RR. The possible maximum and minimum estimates from each study represent the upper and lower 95% CI for the OR (appendix 1). The final column links the PAR to deaths from oral cancer to estimate the number of deaths due to ST.
Between 0 and 1000 or more oral cancer deaths in the US may be attributable to ST use each year; for Sweden this is lower (between 0 and 60) but in India it is very high with over 10 000 deaths from oral cancer possibly attributable to ST use alone. This clearly reflects the large population of India compared with the US or Sweden, as well as higher mortality rates. Table 2 highlights the importance of the relationship between ST use and CVD; the Swedish cohort study by Bolinder et al64 suggests that, in the “worse case”, up to 3000 fatal heart attacks in men (27% of annual number of deaths from heart disease in men) could be attributed to snus use but, in the “best case”, this may scarcely be above zero.
These tables should be interpreted with extreme caution as the 95% CI and range of possible estimates are often quite wide. Although these studies met our “minimum” quality criteria, some still have many limitations. The estimates may not be fully adjusted for possible interactions with cigarette smoking and should be considered extremely “crude”. As case-control studies they may be subject to a number of other biases. Many of the studies do not agree, hence estimates ranging from zero to high numbers of US deaths attributable to ST use are equally plausible. They highlight the uncertainty in the literature, particularly for CVD.
DISCUSSION
Limitations
Inadequate descriptions of ST use
The epidemiological evidence surrounding the health outcomes of ST use is not easily interpretable. Most of the US studies were not designed to consider this, have severe power limitations, and cannot estimate even a rough risk. A detailed description of ST use is often not available, sometimes the only variable is “ST use, ever or never”. Assumptions then have to be made about the types of ST being used. Dose-response relationships provide strong evidence of causality and were especially important in early studies investigating the relationship between cigarette smoking and lung cancer or CVD.84 Few studies have reported detailed analyses of important variables such as frequency or years of use.
ST types are highly variable between and within regions. It is unclear whether results can be generalised elsewhere, although consistent findings of risks associated with oral tobacco in any form are a cause for concern. The types of ST in use have changed considerably over the past few decades, resulting in substantial reductions in the levels of carcinogens. Manufacturers in the US and Sweden report continuing research to reduce these levels. In India the use of locally produced tobaccos has been partially replaced by commercially produced “pan masala”. Future STs may therefore differ from those in use today. Some years must elapse for the health impacts of the newer types to be established.
Validation of ST use
Few studies attempted to validate ST use, biochemical validation being reported in just two cross sectional studies among baseball players in the US. Some studies of cigarette smoking have suggested that self-reporting is reasonably accurate when compared with biochemical markers of tobacco inhalation,85 but research has found that self-reporting is less accurate for patients diagnosed with CVD,86 and this may also apply to other diseases. Validation of daily or weekly usage may be feasible by direct measurement, but only one study reported such an attempt.87
Control of confounding
Many studies reported very little control of confounding, frequently by matching and limited to age groups and sex. Cigarette smoking will be a critical confounder as most ST users also smoke, and this is a more powerful risk factor. The confounding effects cannot be fully controlled by simple analyses of cigarette smoking and require a detailed analysis of smoking history and habits including cigarettes smoked daily, years of smoking, brands used, and inhalation. Other important confounders have also been missed in many studies including alcohol, dietary factors, and socioeconomic status.
Observational data
Most studies were case-control, the only logical design where both the outcome of interest (cancer types such as oral cancers) and exposure (ST use) are rare. With any case-control study there are difficulties in choosing appropriate control series and recall biases may be hard to avoid. A few prospective cohort studies have reported on ST use but, outside India, these require extremely large sample sizes and long follow up periods. Significant loss to follow up may result and misclassification bias may become a significant problem. Some initially classified at baseline as non-ST users may commence use and, conversely, some ST users may give up or start using other tobacco products (particularly cigarettes). Only one prospective cohort study attempted to look at possible changes in exposure over time.
Main findings
Oral cavity cancers in India
There is a substantial risk of oral cancers associated with the types of ST used in India (chewing betel quid with tobacco). Studies from different regions with varying chewing practices have consistently found statistically significant and clinically important ORs associated with betel and tobacco chewing. Many also found clear trends with increased consumption—that is, dose-response relationships. It is likely that around 10 000 annual deaths from oral cancer in India can be attributed to ST use (table 1).
Oral and oropharyngeal cancers in the US
Recent studies have often found no association between ST use and oral or oropharyngeal cancers, and there is some suggestion that tobacco manufacturers may have reduced levels of carcinogenic TSNAs (Jaffe J, Star Scientific Inc, personal communication, 2002). However, the number of ST users is almost always small,88–92 and these studies do not have sufficient statistical power to demonstrate an effect unless the risk is huge. A recent US study88 reported that prior ST use was similar between cases and controls (OR 1.0, 95% CI 0.4 to 2.3), but only 19 cases and 28 controls used ST out of a total sample size of 284 cases and 477 controls. At least 373 cases and 634 controls would be required to have adequate power (80%) to detect a statistically significant (and clinically important) OR of 2.0 when the exposure (ST use) is this rare. This would increase to 1194 and 2030 cases and controls, respectively, to detect a more modest OR of 1.5. Most recent US studies have not been able to address this question.
Oral and oropharyngeal cancers in Scandinavia
The situation in Sweden is different from the US as ST use is much more common. Swedish snus also differs from US ST and tends to have lower levels of TSNAs, although US levels may also be decreasing. However, the incidence of these cancers is low and studies still tend to lack statistical power. Recent studies have not found significantly raised risks for current users, ever users, or ex-users of ST, but none are statistically significant and 95% confidence intervals are very wide. The risks are much higher for ex-users than for current users, which may suggest that early disease symptoms provoke some to quit. Although these findings are consistent with no effect, the studies do not have sufficient power to detect a moderately raised OR.
Dental diseases
Some studies have suggested a possible relationship between ST use and periodontal disease or dental caries, but there are relatively few cross sectional studies with many limitations. A recent study of US men found an increase in dental caries among chewers of tobacco, which may have added sugars.76 One Swedish study also found an increase in dental caries among teenagers using oral snuff in Gothenburg.
Cardiovascular disease
In one prospective cohort study64 an association was found between ST use and CVD mortality. The study population comprised construction workers, which raises questions about generalisability. No statistically significant associations were found in two population based case-control studies. More research is required, especially from other parts of the world with different ST habits. This is potentially critical as CVD is one of the most common causes of death in the world,93,94 and even a small increase in risk could result in many deaths (table 2).95,96
Other cancer sites
No strong association was found between ST use and most other cancers, except for one Asian study of penile carcinoma.67 The use of ST was found to be a risk factor for histologically verified pancreatic cancer in a Scandinavian study,97 and there is some evidence that it may be a possible risk factor for oesophageal cancer.
What is required in the future?
Further studies with sufficient power and adequate control of confounding are required to elucidate the role of ST use. Studies would benefit from improved validation, trend information, and consideration of individual brands. More information is urgently required on the potential health effects of ST use other than cancer, particularly CVD.
A difficulty in many countries has been obtaining sufficient numbers of ST users to enable precise estimates of risk. Populations with high ST use (such as US baseball players) need to be identified and followed over time. One possibility is to set up a multicentre case-control study with centres in different regions such as the US, Sweden and other Scandinavian countries, India and other parts of Asia. There is some evidence that cigarette smokers have quit to become ST users, and some are promoting this as a method of “tobacco harm reduction”. Long term follow up of populations of smokers who either quit tobacco use or become ST users should be established to compare the differences in a range of health outcomes between these two groups. Only further well designed epidemiological studies with adequate sample sizes will be able to resolve these controversies.
Acknowledgments
Clive Bates, Greg Connolly, Karl Fagerstrom, Prakesh Gupta, Alison Hill, Jerry Jaffe, Scott Leischow, Paul Nordgren, Lesley Owen, David Sweanor, Robert West, Margaret Whitehead, Deborah Winn all provided further information or constructive comments. The authors thank Gill Doran for secretarial assistance. The review was funded by the Health Development Agency, UK.
REFERENCES
Supplementary materials
. Web-only Appendix
Files in this Data Supplement:
- [View PDF] - Tables of studies included