Article Text

Statistics from Altmetric.com
Can you scare people out of smoking? Since Janis and Feshbach’s influential research on the use of fear in dental hygiene education in the early 1950s,1 several generations of health educators have often uncritically accepted as near holy writ that you should not try to scare people into healthy practices, including smoking prevention and cessation.2 3 Given that survey evidence from ex-smokers has repeatedly affirmed that personalised concern about “scary” health consequences is the primary motivation ascribed to smoking cessation4-6 and is associated with predictors of cessation,7 interesting questions arise about whether this dogma is empirically grounded or whether it rather reflects a profession-wide neurosis intent on avoiding opprobrium from those who believe it is somehow not “nice” to deal in gory imagery in the name of persuasion.8
A mass media-led campaign launched in Australia in June 1997 has been seen by many as “the mother of all scare campaigns” (see the illustrations on the cover of this issue of Tobacco Control, the figure in this essay, the campaign-related material on the world wide web at <http://www.quitnow.au>, and the description of that web site on page 89). The television advertising campaign has been described repeatedly as “hard-hitting”, “gory”, and something smokers will “see once and never forget”. It has since been used by the state of Massachusetts tobacco control programme9 with dozens of other international enquiries also having been received.
To some, the campaign might be seen as something of a health promotion profanity in the wake of recent so-called “positive” practice—for example, campaigns using every manner of non-smoking role model; general proselytising about “healthy lifestyles”, freshness, and so on). However, to others it represents the culmination of a painstaking formative research process undertaken in the context of a stalled decline in smoking prevalence and an historical retreat from the more hard-hitting Australian campaigns of the early 1980s.10The events, evidence, and arguments behind the campaign’s development may be of interest to readers of Tobacco Control.
In 1996, the Australian federal minister of health, Dr Michael Wooldridge, appointed a small ministerial tobacco advisory group (MTAG), which included in its membership experts in tobacco control research, campaigns, and tobacco policy. MTAG was asked, in partnership with existing state-based programmes, to develop a new and relatively well-funded campaign which would spend approximately US$0.30 per head of “new” money in a 12-month period. MTAG’s strategic advice to the minister was to focus on smokers aged 18–39—that is, to conduct a cessation campaign, not a prevention campaign. Why? While the political risk-benefit ratio of a transparently teenager-directed campaign would be favourable for a minister of health, the risk-benefit ratio in terms of effectiveness among teenagers themselves was likely to be very different.11 12 Worse than simply being ineffective, teen campaigns carry greater risk of backfiring: (“Why pick on kids when so many adults smoke?”, “Your attempt to do a ‘cool’ campaign to persuade us is pathetic.”). To his credit, the minister accepted the advice to target the 32% of Australians aged 18–39 who smoke.13 This cessation-first strategy was subsequently to be strongly endorsed at the opening plenary session of the 10th World Conference on Tobacco or Health in Beijing in Richard Peto’s analysis of where the greatest payoff for tobacco control lies.
In most health campaigns driven by advertising agencies, the first step is to talk to the market (“we need to do focus groups to learn why people smoke”). Instead, MTAG decided to review what was already in hand—40 years of psychological research and more than a decade of largely unpublished market research reports commissioned by various Australian state Quit campaigns. More than 100 of the latter were identified, providing at little cost an invaluable perspective for deciding the approach that was to be taken. In what was arguably a simplification of the stages of readiness-to-change behaviour,14 the brief to the advertising agency proposed an individual model based on the “personal agenda” about smoking. The model assumed the following: (a) the day-to-day actions of individuals are largely explained by the existence of an unwritten personal agenda with items on it implicitly ranked for importance/urgency and grouped along the following lines: today, tomorrow, sometime soon, if I ever get the chance, when I eventually get around to it; (b) for intentions to become actions they must at least make it to today’s agenda; and (c) behaviours (like quitting smoking) that require action over many days and which are difficult, require resources and reinforcements external to the individual.

{kind=link}
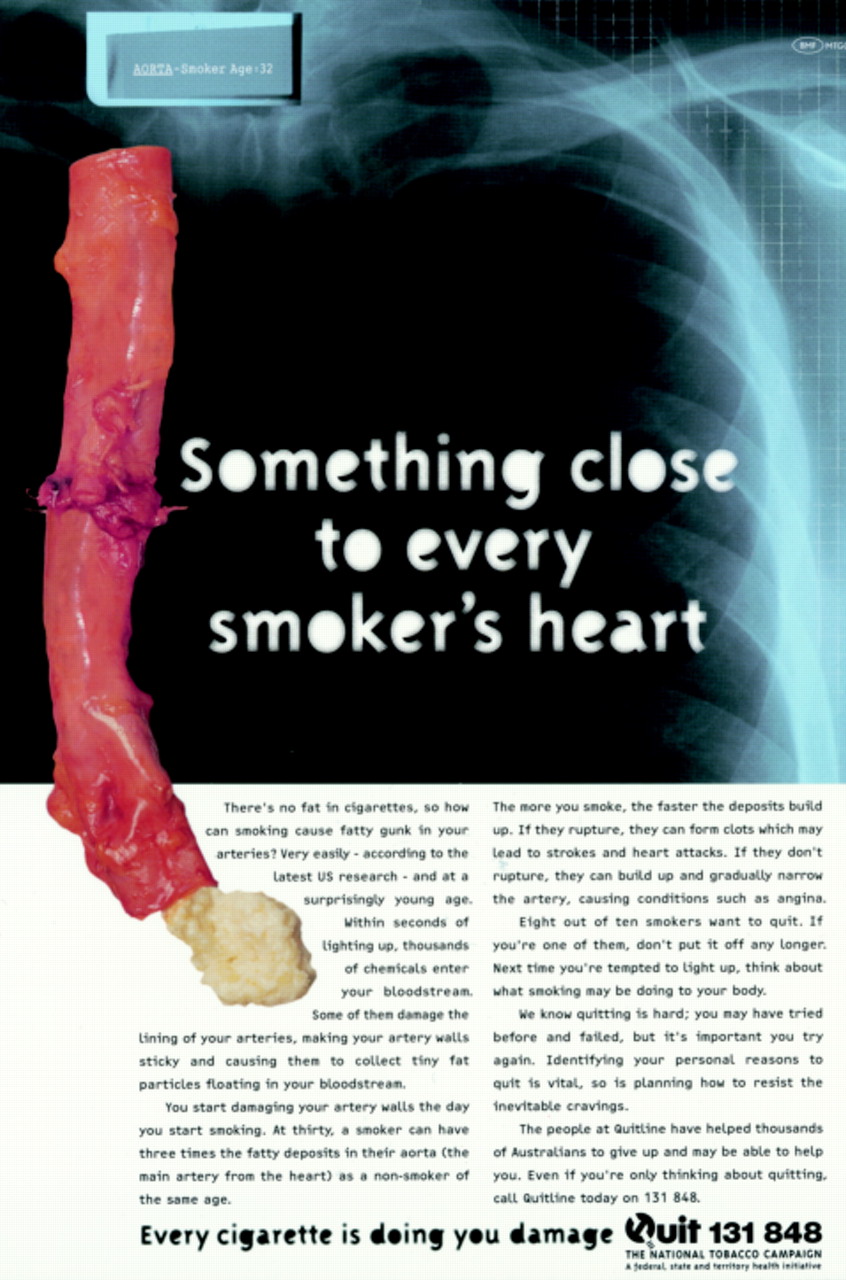
The “Aorta” advertisement.
It was known that most smokers “intend” to quit,15 but clearly for most smokers, for most of the time, quitting is not on today’s agenda. Hence the major communication objective in the brief to the agency was that the campaign should elevate quitting on smokers’ personal agendas.
The brief also listed seven key facilitators of behaviour change. It stated that to potentiate an existing intention, an individual should be stimulated toward some or all of the following. He or she should: (a) gain fresh insights on the recommended behaviour; (b) reassess the importance of the behaviour; (c) reassess theurgency of carrying out the behaviour; (d) reassess thepersonal relevance of the behaviour; (e) have confidence in their own ability to carry out the behaviour (self-efficacy); (f) remember or be reminded to do it; and (g) for long-term change, gain more than is lost by carrying out the behaviour (response efficacy).
Further, taking account of results of the review of the qualitative research undertaken, the campaign should: (a) show the damage of smoking in new insightful ways that are both enlightening (“Now I see what the doctors are on about”) and chilling (“I can’t bear to think of that happening to me”); and (b) develop a conditioned association between the images of bodily harm and the act of smoking such that those images are evoked when smoking is contemplated or seen. Unlike traffic accidents where people “know” the mechanisms of cause and effect, knowledge of the serious consequences of smoking are known to most smokers only in the abstract. Most know the long-term effects of smoking only because they have been told third-hand what scientists have discovered about it. People have a poor ability to perceive, understand, evaluate, and respond to statements about risk.16 The evidence about smoking is often stated in probabilistic terms, but we know this lets people distort and objectify the hazard, and “exempt” themselves with various rationalisations.17 Past campaigns may, paradoxically, have been weakened by emphasising how “risky” smoking is. Given that people are more likely to act on the basis of what they experience than what they are told, the communication challenge for this campaign was to translate the scientific knowledge about smoking into “felt” experience, rather than cognitive appreciation of risk.
Because people do not think probabilistically or behave “rationally” in relation to probabilities,18 it may be more effective to describe the certain consequences of smoking, even if they are less dire than the uncertain ones, such as lung cancer and heart attacks. This was a core rationale behind the content of the campaign as executed.
To convey the doctor’s eye view of the damage caused by smoking, it was felt important to bring the advertising agency’s creative team in direct and extended contact with medical specialists. This was done in “expert workshops”, according to the following formula: meet in the evening, allow plenty of time, provide good food and wine, and prime the agency to press relentlessly for images and words that describe disease processes due to smoking, particularly little or unknown aspects. The workshops began predictably, with well-intentioned medical experts telling the creative team how to make advertisements that would work, or more commonly, telling them that nothing would work! But persistence from the creative team yielded dividends, best exemplified by the cardiologist who finally said of atherosclerotic damage: “I suppose you could liken a severe case of atherosclerosis to squeezing Brie cheese from a toothpaste tube, except it’s an artery”. And so was born the advertisement known as “Aorta”, illustrated on the cover of this issue of Tobacco Control, in the figure, and on page 89.
“Aorta”, which features “gruel” (fatty deposits) being squeezed by a surgeon’s gloved hand from a human aorta, is one of a set of three television advertisements in the campaign,19 the others covering emphysematous damage and the recent discovery of a mechanism by which smoking damages the P53 tumour suppressor gene in lung tissue.20 Each advertisement brought smokers some “new news” about smoking, but more than this the message was framed in a way to maximise the effect on behaviour.
First, the emphasis was on relatively certain rather than less probable effects. Perhaps heavy emphasis in the past on risk has inadvertently encouraged smokers to take a chance. So the campaign slogan was: “Every cigarette is doing you damage”, with the advertisements focusing upon continuing damage (the things that happen as you smoke now, rather than clinical outcomes). Second, because beliefs about consequences of actions are only able to determine behaviour if they are salient (top of mind) at the time the behavioural decisions are made,21 22 a device was needed to bring these consequences to mind at the time smoking was contemplated. To achieve this, the advertising agency (Brown Melhuish and Fishlock) created a journey into the lungs. The viewer, as in virtual reality, travels with the smoke as it is inhaled down the trachea and into the lungs where it begins its deadly work. This scene in each of the advertisements immediately follows a brief typical moment in which the smoker lights up and inhales, ignorant, it seems, of the damage being done.
Great care was taken in crafting these “smoker moments” to maximise their ability to engage the smoker and convey empathy for the smoker’s situation. Pre-testing of this component showed that smokers are mildly self-deprecating in relation to their smoking and respond empathically to depictions of awkward “desperate” smoking situations, such as a smoker reduced to lighting a cigarette from the flame of a gas stove (see top left panel on the cover). The advertisements will work to the extent that the thought, act, or sight of inhaling a cigarette brings to mind the sticky walls of arteries, genetic damage to lung tissue, or the “rotting” that characterises chronic lung disease. Extensive quantitative testing of the “Aorta” advertisement in particular showed that the pictures produced a strong visceral “yuk!” response, hence qualifying it as a “fear appeal”.
Fear or threat appeals have great potential for stimulating behavioural change, if used correctly.23-25 Fear is the negatively valenced emotion that may be felt by a person exposed to a threat appeal. It can be dealt with adaptively by a behavioural response that removes the reason to be fearful, such as quitting smoking, or maladaptively by a psychological response meant to dispose of the fear—for example, denying the truth or personal relevance of the message. To maximise the chance of the intended behavioural response, each advertisement carried a Quit Helpline number. Smokers who were stimulated to quit, but wanted assistance, could (and did in large numbers) contact a recently upgraded telephone counselling service.
Over the first six months, the television campaign reached 95% of the target population with an average frequency of nine exposures. There was a lower socioeconomic bias in choice of media placement to reflect the social class gradient of smoking in Australia.
By the time this essay goes to press, the jury will still be out on whether this campaign “worked”. Indeed, it would be naive to expect any one intervention to “work” in isolation from surrounding cultural influences and other contemporaneous variables.26 27 However, there are early signs of processes and outcomes that suggest things are going to plan. The weekly tracking survey throughout the six-month campaign showed that the campaign had high impact, stimulated much family and workplace discussion about smoking, and increased activity towards quitting. This is much more than can be said about reaction to the all-too-typical “positive” campaigns where recall and evidence of community discussion have been found to be relatively low.28 29What is now needed is public health support and the political will for a significant ongoing comprehensive programme, together with realistic funds at least equal to what the government gets in tax revenue from the illegal sale of cigarettes to minors (which in Australia would amount to nine times the budget of the recent campaign).30
References
Note to readers
We hereby solicit your ideas and contributions for future covers of Tobacco Control. As with previous covers, we would like future covers to be colourful and creative—with a tobacco control theme. Original artwork, anti-tobacco posters, photographs, and cartoons may all be considered. Material with an international flavour would be particularly desirable. A cover essay will generally appear in each issue to provide appropriate background information and commentary on the cover.
Please send ideas and submissions (original or high-quality, camera-ready photographs) to the editor at the address on the inside front cover.—ed