Article Text

Statistics from Altmetric.com
Timor Leste: world’s largest graphic health warnings
The journey of tobacco control in Timor-Leste dates back to 2004, just two years after the country became independent in 2002. Timor-Leste ratified the World Health Organization’s (WHO) Framework Convention on Tobacco Control (FCTC) in December 2004, which came into force in March 2005.
All articles written by Marita Hefler unless otherwise attributed. Ideas and items for News Analysis should be sent to: marita.hefler@menzies.edu.au
The ratification of the FCTC, however, did not immediately translate into effective measures for tobacco control. A breakthrough in tobacco control was the decree-law passed in 2006 which dealt with health warning labels, tax control of manufactured tobacco products, and customs duties. Although the law is testament to the Government’s commitment to tobacco control in the island nation, implementation remained a formidable challenge and was admittedly lax given the lack of resources and limited technical capacity. The passage of the first decree law in 2006 was followed by a number of other laws; however, implementation remained weak.
In 2006, the Ministry of Health (MoH) conducted the first-ever Global Youth Tobacco Survey (GYTS) which revealed alarmingly high youth tobacco use prevalence at 41%. The subsequent Noncommunicable Diseases (NCD) STEPS survey in 2014 showed tobacco use prevalence among male adults was 70%. This evidence opened doors for tobacco control advocacy at the highest political level, resulting in the passage of comprehensive tobacco control legislation in 2016. This was the beginning of a wide range of tobacco control measures – community engagement, dissemination of NCD STEPS findings, and most importantly, the enforcement of tobacco products packaging provisions laid out in the law.
The tobacco control law was a watershed moment in the public health sphere, given the inordinately high prevalence in such a young country with a nascent health system and a large proportion of young people. The then Prime Minister and two times health minister Dr Rui Maria de Araujo, under whose tenure the tobacco control movement gained momentum, became the face of the anti-tobacco campaign in the country. His contributions were acknowledged at the global level when he was awarded the WHO World No Tobacco Day Award in 2016 for having played the crucial role in the passage of the legislation for tobacco control. Dr Rui not only exhibited exceptional political commitment for tobacco control but walked the talk, as he quit smoking himself and eventually became a formidable advocate.
Soon after the promulgation of the tobacco control law, the (MoH) requested WHO to assist in designing the graphic health warnings (GHWs) for cigarette packs to be implemented as per provisions under the law. An intensive process to choose suitable and strong warnings was initiated under the leadership of WHO Representative to Timor-Leste Dr Rajesh Pandav who capitalised on this opportunity to bring the country to par with other countries in South-East Asia and also at the global level in implementing Article 11 of the WHO FCTC. The first GHW was designed in September 2016, and over the course of the next 12 months, WHO and the MoH together refined various versions of the chosen designs to gain maximum leverage through strong anti-tobacco messages to convey the harmful effects of tobacco and secondhand smoke.
Today, six GHWs appear on cigarette packages, covering oral cancer, lung cancer, impotency, abortion, cardiovascular diseases and chronic lung disease. The GHWs implemented by Timor-Leste place the country at the highest level of achievement under Article 11 of the WHO FCTC and is just below plain packaging, as recommended by WHO and implemented by few countries in the world.
The law mandates that every tobacco package must carry health warnings in the form of pictures and text. The GHW and the text are required to cover 85% of the front side from top to bottom and 100% of the back of the tobacco package. On one lateral side, information related to toxic emissions is to be mentioned covering 50% of the side (white text on black background).
The tobacco companies have adhered to the 6 September 2018 deadline for the new health warnings on tobacco packages. Furthermore, beginning 6 November 2018, no retail or wholesale store/entity can store, display or sell any tobacco products which do not comply with the mandatory warning regulation.
From 2004 to the present day 14 years later, the journey of tobacco control has not been easy. However, Timor-Leste has demonstrated commendable political commitment and willingness to curb the menace of tobacco given its high prevalence. This also is an excellent example of collaboration and partnership with the Government and WHO for effective tobacco control in challenging situations. The country has implemented these measures in a comparatively short time compared with many other countries. Sustaining the gains and ensuring that no tobacco products are being sold without the mandatory health warnings in the country will be the new challenge.
Frederico Bosco
Helder Juvinal Neto da Silva
Mario Serekai
Ministry of Health, Timor Leste
frebosco@yahoo.com
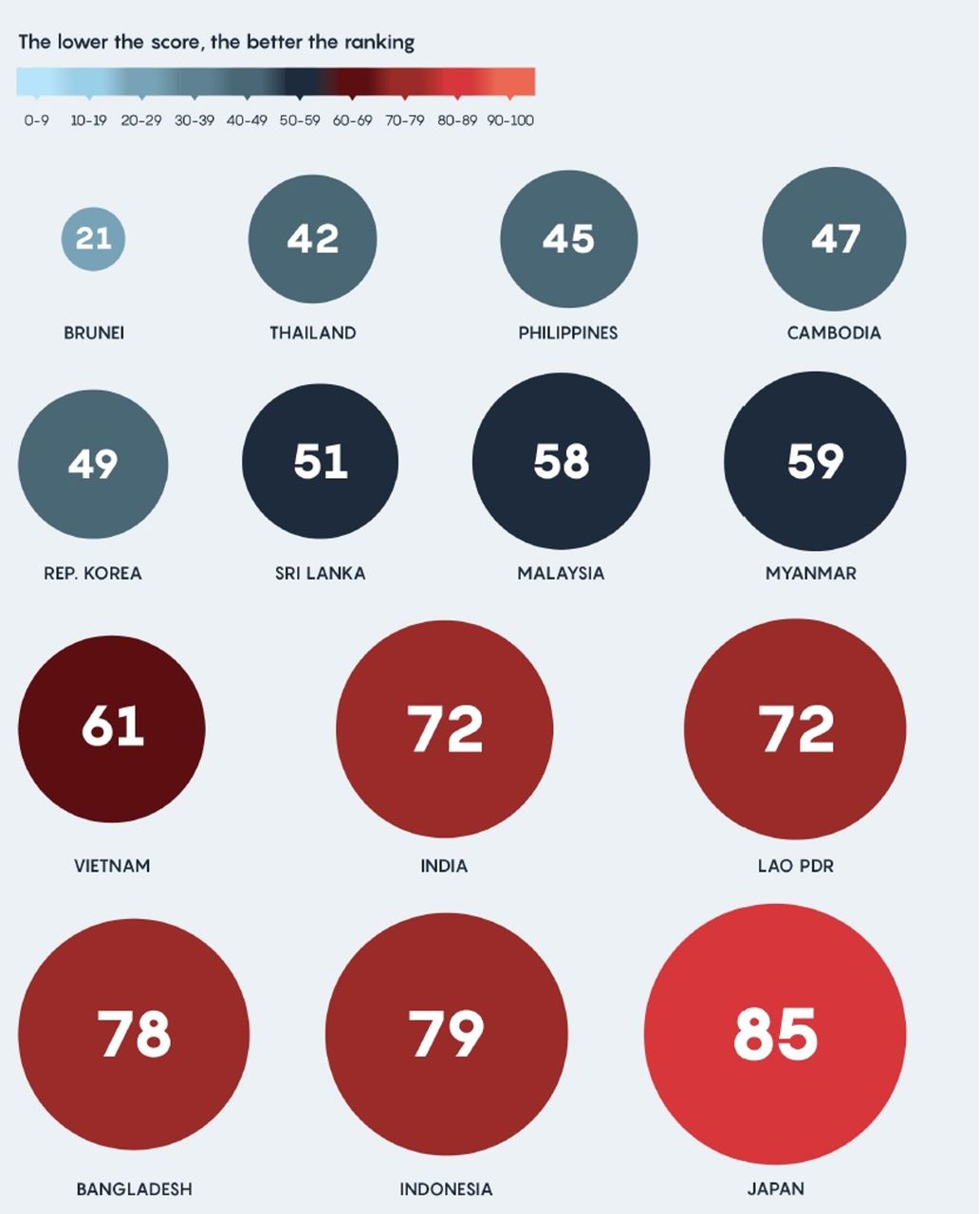
Asia: 2018 tobacco industry interference report on 14 countries

Country rankings for the 14 countries assessed as part of the Asian Tobacco Industry Interference Index. The larger, the dots, the higher the level of interference.
The first Asian Tobacco Industry Interference Index was published in September 2018 by the Southeast Asia Tobacco Control Alliance (SEATCA). Previous reports have included countries in the ASEAN region; the 2018 report for the first time has been expanded to include Japan, India, Bangladesh, Sri Lanka and the Republic of Korea.
The report found that while there is enormous room for improvement, there are some significant achievements and examples of strong leadership. One bright spot is Thailand’s requirement for tobacco companies to submit a full report about business expenses including marketing, production volume, market share and income. It is the first Asian country to introduce this measure. In Indonesia, one of the few countries in the world which is not yet a party to the FCTC, progress is also being made, with the Ministry of Health having adopted guidelines for managing conflict of interest with the tobacco industry.
The Vietnamese government is the only government in the Asian region, and one of only two globally, to have announced a policy of non-engagement with the Philip Morris International-funded Foundation for a Smoke Free World. In January 2018, the Polish government also announced it will not engage with FSFW or consider FSFW-generated research in policy making. The stance is in line with the recommendation of the WHO and numerous health and non-government organisations, as well as many universities in the USA, Canada, Europe, Australia and New Zealand.
Overall lack of full transparency in disclosing transactions with the tobacco industry remains a significant problem in most countries surveyed. Countries do not have registers of tobacco industry entities and affiliate organisations. This is a significant issue given the tobacco industry’s long history of using front groups and third parties to represent its interests, as well as the more recent creation of the Philip Morris-funded Foundation for a Smoke Free World (FSFW).
Corporate social responsibility (CSR) activities are also a significant problem, not only as a form of proxy advertising, but more importantly as a channel to access senior government officials. Benefits to the tobacco industry such as duty exemptions, subsidies and delayed introduction of measures such as health warnings also undermine tobacco control in the region. As in other regions, the ‘revolving door’ between government roles and the tobacco industry are problematic, as are lack of prohibitions on political donations from the tobacco industry.
Overall, Brunei, Thailand and the Philippines are the best performers in the Asian region, while Japan, Indonesia and Bangladesh are ranked worst. Among the recommendations in the report are the need to boost transparency around necessary meetings between the tobacco industry and governments, restrict tobacco industry participation in policy making, and ban CSR activities.
The full report can be downloaded at: http://seatca.org/dmdocuments/SEATCA_TI_Interference_Index_2018.pdf.
Bangladesh: First country report on tobacco industry interference

{kind=link}
{kind=link}
The first Tobacco Industry Interference Index for Bangladesh was published in September 2018. Bangladesh was found to have the third highest level of tobacco industry interference of 14 countries surveyed.
In addition to its inclusion in the Asian Tobacco Industry Interference Index, a stand-alone country report was also published in September 2018 by PROGGA – Knowledge for Progress, a non-profit organisation for research, advocacy and capacity building, with technical assistance from SEATCA. The report was launched in collaboration with the Anti-Tobacco Media Alliance for tobacco advocacy. The index is the first of its kind in Bangladesh.
The government of Bangladesh adopted the FCTC Article 5.3 Guidelines in 2008 which provide specific measures to protect government policymaking from tobacco industry interference. FCTC Article 5.3 is the key weapon to protect a country’s tobacco control measures and policies from the vested interests of tobacco companies. Although almost a decade has already passed, the policy based on the Guidelines is yet to be formulated in Bangladesh.
The report found that the although the Ministry of Health and Family Welfare and National Board of Revenue are implementing tobacco control measures, tobacco industry interference is happening through a pro-tobacco think tank which has influenced the Ministry of Agriculture and the Ministry of Finance. The strategy of targeting ministries outside the health sector is in line with tobacco industry strategies elsewhere, particularly as countries have increasingly implemented FCTC measures. Corporate social responsibility programmes are also a significant issue, and have included the Agriculture Secretary, Labour Secretary and Finance officials, who are members of the British American Tobacco CSR committee.
Another major issue is benefits granted to the tobacco industry. These include changing the position of graphic health warnings to the lower rather than upper portion of tobacco packages, favourable production conditions for British American Tobacco (BAT), with reduced salaries and benefits to workers, tax waivers in export processing zones, and tax benefits for unprocessed tobacco.
As with other countries, unnecessary interactions and lack of transparency around meetings between government officials and tobacco industry representatives remain problematic. Of particular concern, several high-level government officials hold positions in BAT Bangladesh. The report also notes that tobacco companies are given awards for merely complying with the law regarding tax payments. At the award ceremonies, high-level government officials in the finance and industry portfolios attend, creating a direct access avenue for tobacco industry executives.
The full report can be downloaded at: http://www.tobaccoindustrywatchbd.org/contents/uploaded/TIIIndexBangladesh2018FullReport.pdf. A fact sheet is available at: http://www.tobaccoindustrywatchbd.org/contents/uploaded/FactSheetNewEnglish.pdf.
New zealand: Foundation for a smoke Free world funds new centre
The New Zealand government has become the first which will need to consider how to handle the multiple layers which obscure transparency of PMI as the ultimate funding source of initiatives spawned by FSFW. In September 2018, the ‘Centre of Research Excellence: Indigenous Sovereignty and Smoking’ was launched in Auckland.
On its website, the mission of the centre is stated as ‘…to support indigenous aspirations to flourish as individuals, families, tribes and nations who are recognised as sovereign people’. It includes a statement that it is funded by an FSFW grant, however there is no mention anywhere of PMI as the sole funder of FSFW. Many Māori leaders will recall PMI being forced into a rare apology in 2006 after using Maori images on Israeli cigarette packets. The company was heavily criticised for misappropriating and exploiting Maori culture.
The centre was headlined in the publication New Zealand Doctor (aimed at general practitioners and primary health staff) as ‘Proceeds of tobacco pay for research into indigenous smoking cessation’, a title which fails to convey the fact that the scope of FSFW funding is set sufficiently narrowly to serve PMI’s commercial interests. Also neglected in the coverage of the centre and on its website is the length of time it took for tobacco plain packaging to be introduced in New Zealand, 6 years after it was first mooted. The threat of litigation, as happened in Australia, has been suggested as the most likely cause of the delay.
The director of the centre was quoted by New Zealand media as planning to partner with indigenous organisations and researchers around the world, presenting a challenge not only for the New Zealand government, but also for other governments and organisations concerned with adhering to Article 5.3 of the FCTC to protect policy making from tobacco industry interference. Other governments would do well to follow the lead of Vietnam and Poland to issue clear policies of non-engagement with FSFW and its sub-organisations. These could include not taking into account FSFW-generated research in policy making, disallowing government funding to organisations which also receive funding from FSFW, and ensuring that meetings between government officials and FSFW-funded personnel are limited and/or publicly disclosed.
Guam: Tobacco tax increase a double win for health and revenue
On August 23, 2018, Guam, an unincorporated Territory of the Unites States of America, raised tobacco taxes from $three to $four per pack of 20 cigarettes, with commensurate increases on other tobacco products. This places the tiny Pacific Island of 160 000 people fourth among all US States and Territories in terms of tobacco tax rates.
The tobacco tax increase was welcomed by the public health community as a strong policy measure to curb tobacco consumption. Despite declines in tobacco use, smoking and other forms of tobacco use remain high in the island; one in four adults and one in seven high school students are current smokers. However, the process to securing the tax increase was a contentious and challenging one for health advocates.
The tax increase was first introduced in 2017, as a bill to reduce tobacco consumption and generate funds for tobacco use prevention, cessation and surveillance. Despite strong public support from local, regional and international stakeholders, it failed to pass in the face of opposition from powerful political families who control the tobacco retail industry on the island.
The opportunity to re-introduce the tax increase arose when the Legislature was crafting the island’s 2019 budget bill; US federal tax cuts made it imperative to identify new sources of revenue to compensate for projected revenue shortfalls. Raising tobacco taxes became one of the strategies identified by the Legislature to augment government income. Despite the fiscal advantages, several attempts were made to delete the tobacco tax increase from the budget bill. The concerted advocacy and vigilance from community advocates proved crucial to the survival of the proposed tobacco tax increase. Local data on the magnitude of the tobacco epidemic, its socioeconomic impact on the island community and the documented declines in tobacco use following previous tax increases were pivotal to securing the support of a majority of the Senators. The Bill was passed at the Legislature on August 10 and transmitted to the Governor’s Office. The Governor vetoed the Bill on August 11; however, the Legislature amended the Bill and re-submitted it to the Governor. The Bill lapsed into law on midnight of August 23, 2018.
The tobacco tax increase is anticipated to generate about $9.35 million in 2019, comprised of $8.89 million from cigarette sales, and $0.46 million from cigars and other tobacco products. A portion of the tax revenues is earmarked for Guam’s Healthy Futures Fund, which supports the Guam Memorial Hospital and tobacco prevention and cessation programmes of the Department of Public Health and Social Services and the Guam Behavioural Health and Wellness Centre. Tobacco tax revenues also fund the Guam Cancer Trust Fund and the Guam Cancer Registry. Thus, the tax increase represents both a public health win and a fiscal victory for the island community.
As part of the United States, which remains a non-Party to the International Framework Convention on Tobacco Control (FCTC), Guam has had to rely on local government action to curb the tobacco epidemic. The members of the Guam Noncommunicable Disease Consortium, Tobacco Control Action Team, lauded the tax increase as a strategic intervention to reduce the health and socio-economic burden on the island. According to the members: ‘Tobacco use remains the number one preventable cause of death in Guam. Raising tobacco taxes is the single most effective policy to reduce tobacco use. This tax increase will save lives, reduce the tobacco burden and help our island community generate more income for our prevention and cessation programmes. Even if Guam is outside the FCTC Conference of Parties, we will continue to pursue evidence-based tobacco control measures through local leadership, good data and advocacy.’
Annette M. David
Guam State Epidemiological
Outcomes Workgroup
amdavid@guam.net
Cathy R. Castro
American Cancer Society
Cancer Action Network
Elizabeth Guerrero
Guam Department of Public Health
and Social Services