Article Text

Abstract
Objectives To assess indoor secondhand smoke (SHS) exposure in restaurants and bars via PM2.5 level measurements in five cities in China.
Methods The study was conducted from July to September in 2007 in Beijing, Xi'an, Wuhan, Kunming and Guiyang. PM2.5 concentrations were measured in 404 restaurants and bars using portable aerosol monitors. The occupant density and the active smoker density were calculated for each venue sampled.
Results Among the 404 surveyed venues, 23 had complete smoking bans, nine had partial smoking bans and 313 (77.5%) had smoking observed during sampling. The geometric mean of indoor PM2.5 levels in venues with smoking observed was 208 μg/m3 and 99 μg/m3 in venues without smoking observed. When outdoor PM2.5 levels were adjusted, indoor PM2.5 levels in venues with smoking observed were consistently significantly higher than those in venues without smoking observed (F=80.49, p<0.001). Indoor PM2.5 levels were positively correlated with outdoor PM2.5 levels (partial ρ=0.37 p<0.001) and active smoker density (partial ρ=0.34, p<0.001).
Conclusions Consistent with findings in other countries, PM2.5 levels in smoking places are significantly higher than those in smoke-free places and are strongly related to the number and density of active smokers. These findings document the high levels of SHS in hospitality venues in China and point to the urgent need for comprehensive smoke-free laws in China to protect the public from SHS hazards, as called for in Article 8 of the Framework Convention on Tobacco Control, which was ratified by China in 2005.
- Secondhand smoke
- surveillance and monitoring
- hospitality venues
- environmental tobacco smoke
Statistics from Altmetric.com
Background
Secondhand smoke (SHS) is the combination of smoke emitted from a cigarette or other burning tobacco products and the smoke exhaled by the smoker. SHS is a complex mixture of gases and particles, with particles of fine to ultrafine size ranging from 0.02 to 2 μm.1 These particles can be easily inhaled deep into lungs causing various diseases to multiple systems and organs in humans. Although not specific to SHS, large quantities of respirable particles (RSP) are emitted from burning cigarettes. Xiu et al2 found that indoor RSP levels in offices with smoking occurring were three times higher than those with no smoking. Alpert et al3 also found that 93% of the indoor RSP were attributable to tobacco smoke during active smoking. Measuring the concentration of indoor particles with mean aerodynamic diameter no more than 2.5 μm (PM2.5), which are recognised as a significant threat to public health, offers another assessment of indoor air pollution.4–6
SHS exposure is a completely preventable health risk factor, and there is no known safe level of SHS exposure.7 In May 2003, the member countries of the World Health Organization (WHO) adopted a historic tobacco control treaty, the Framework Convention on Tobacco Control (FCTC). Article 8 of FCTC calls for the expansion of smoke-free places at the national and other jurisdictional levels in signatory countries to protect people from SHS hazards. On 4 July 2007, the second session of Conference of the Parties to the WHO FCTC elaborated Guidelines on Protection from Exposure to Tobacco Smoke to assist parties in meeting their obligations under Article 8 of the WHO FCTC, and to identify key elements of legislation necessary to effectively protect people from exposure to SHS.
In China, there are 350 million smokers. The overall prevalence is 35.8% (66.0% of men and 3.1% of women),8 which means that the risk for non-smokers to be exposed to SHS is very high. Some national prevalence studies in China reported that 53.0% of non-smokers in China were regularly exposed to SHS in 19969 and 51.9% in 2002.8 SHS exposure occurs in various places, and the National Prevalence Survey in 2002 showed 82% of those passive non-smokers reported their SHS exposure happened in homes, 67 in public places, 35% in public places and 35% in workplaces.8
Hospitality venues—restaurants, bars and nightclubs, for example—are both workplaces for hospitality workers and places where the public spend, potentially, a considerable amount of time. Due to the lack of smoking regulations in these kinds of venues in China, hospitality workers and patrons alike are exposed to high levels of SHS. A study conducted in Beijing in 2004 on SHS levels of 14 public places, including five restaurants, showed that airborne nicotine concentration in the five restaurants ranged from 2.07 to 28.72 μg/m3, with median of 4.91 μg/m3, more than 14 times the concentration in hospitals and over seven times that in schools.10 A cross-sectional study of SHS in 92 restaurants and bars in Beijing, China, in 2006 showed that the average of the indoor PM2.5 levels in venues where smoking was allowed was 280 μg/m3, 200% higher than that in venues with smoking restrictions (93 μg/m3).11
In China, objective assessments of SHS exposure are quite limited, especially in hospitality venues. As a party to the WHO FCTC, China is obligated to take effective measures to protect its public from SHS exposure as stated in Article 8. In recognition of its FCTC obligations and as a host of the 2008 Olympic Games, China promised that the Games would be smoke-free. Mostly driven by these two factors, China initiated a series of tobacco control activities in public places including hospitality venues to reduce SHS exposure. This study was aimed to describe a convenient and practical method to assess indoor SHS exposure in China and to provide scientific evidence for the Chinese government to adopt effective measures to reduce or eliminate SHS hazards in hospitality venues.
Methods
Sampling
The study was conducted from July to September in 2007 in five cities in China: Beijing, the capital of China, located in northern China; Xi'an, a city in the Central Western part of China; Wuhan, a city in the Central part of China; and Kunming and Guiyang, two cities in southwest China.
In each city, hospitality venues were sampled from two districts following three steps. First, all the hospitality venues were divided into five categories according to Standards of Industry Classification issued by the National Statistics Agency of China, which are Chinese restaurants, Chinese fast food restaurants, Western restaurants, Western fast food restaurants and bars.12 Second, venues were sampled from each of the five categories in the ratio of 10:1:1:1:3 according to the number of restaurants and bars listed on website yellow pages. Fifty Chinese restaurants, five Chinese fast food restaurants, five Western restaurants, five Western fast food restaurants and 15 bars were selected in each city. Third, restaurant size and average expenses per patron per visit according to the owners' reports were taken into account to keep a balance to some extent in these two aspects for the sampled venues. Via this three-step procedure, a total of 405 hospitality venues were selected and surveyed in the five cities.
Instruments and measures
Fine RSP, or PM2.5, was used as the proxy measure for SHS. Data collectors in each city were trained directly to use a standard measurement protocol, which was consistent to the method detailed in the web-based training course (http://www.tobaccofreeair.org/) developed by Roswell Park Cancer Institute, New York, USA, and used in previous studies.5 Portable battery-operated aerosol monitors (TSI SidePak AM510 Personal Aerosol Monitor; TSI Incorporated, Shoreview, Minnesota, USA) fitted with 2.5 μm impactors were used to sample both the outdoor and indoor PM2.5 levels of each venue. The airflow rate was set at 1.7 L/min using a Drycal DC Lite flowmeter to ensure proper operation of the size-selective impactor. The calibration factor setting of 0.32, suitable for SHS,5 13 was used, and the monitor was set to 1 min data log interval, which averages the previous 60 one-second measurements. The portable device was calibrated to zero prior to each use by attaching a high-efficiency particulate air filter according to the manufacturer's instructions.
To avoid disturbing people's normal behaviour during sampling, the monitor was placed in a bag with a short length of Tygon tubing attached to the inlet and left protruding on the outside. Logging of PM2.5 levels began at least 5 min outside of a venue before entering to provide baseline measurements. Since the monitor was in a bag worn by a data collector, it sampled the air from the zone around the data collector's waist. After outdoor measurements, the monitor was kept logging data when collectors entered a venue as patrons: they bought some food or drink and stayed for at least 30 min for indoor air sampling, and they tried to find a table as close as possible to the central position of the venue. The bag was placed on the table rather than on the floor or a chair, so that the air being sampled was at the level of occupants' normal breathing zone. The number of patrons and the number of burning cigarettes were recorded at the time of entry into the venue, at the time of exiting and every 15 min during the visit itself. The volume of each venue was calculated by using a sonic device (Zircon Corporation, Campbell, California, USA) to measure each of the linear dimensions of the room. If the room was irregular in shape, making it impossible to measure the volume by the sonic device, then the dimensions and volume were estimated by the trained data collectors. If a venue had a partial smoking ban, then the measurements were taken in the non-smoking area. Time of entering and exiting the venue and observations of occupants' smoking behaviours (eg, number of lit cigarettes) were recorded.
Data analysis
Data from each venue visit was downloaded to a computer using the TSI TRACKPRO V.3.4.1 software. For each venue, the data logged during the minute of entering and exiting the venue were removed so that the remaining data points were either all from the indoor of a venue or all from its outdoor. These were averaged, respectively, to provide a mean PM2.5 level inside or outside the venue. The PM2.5 data from a bar in Wuhan were excluded from analysis due to its unexplainable extremely high indoor PM2.5 level considering the smokers, patron numbers, outdoor PM2.5 levels and other possible PM2.5 sources; thus, data from 404 venues were finally used for analysis.
Because the PM2.5 concentrations were log normally distributed all statistical analyses used log-transformed PM2.5 concentrations. Pearson χ2 tests and Fisher exact tests were used to test proportion differences; geometric means of PM2.5 levels were compared among different cities, different venue types and outdoors versus indoors using analysis of variance ANOVA tests and t tests. UNIANOVA tests were used to compare the indoor PM2.5 levels in different venues with or without smoking observed after controlling for outdoor PM2.5 levels.
The occupant density (OD: the number of occupants per 100 m3) and the active smoker density (ASD: the number of burning cigarettes per 100 m3) were calculated for each establishment sampled. Spearman rho as well as partial correlation analysis were performed to determine the correlations between the OD, ASD, outdoor PM2.5 levels and indoor PM2.5 levels. Also, linear regression models were used to examine the relationship between indoor PM2.5 levels with outdoor PM2.5 levels, ASD, OD, different cities and different types of venues.
Results
Table 1 presents the general characteristics of the hospitality venues where samples were taken in the five cities. The numbers of the five types of hospitality venues in each city were basically consistent with the proportion of 10:1:1:1:3 (described in the Methods section), and Pearson χ2 test (χ2 (16)=1.98, p=1.00) indicated no statistical differences among the proportions of different types of restaurants and bars in different cities. Maximum occupancy at 42.6% of the venues was ≤100 patrons, while 33.2% of venues had a capacity of 101 to 300 patrons. About 44% of the venues had an average expense per patron per visit of 21–50 RMB and one third of venues had an average expense per patron of 20 RMB or lower, which suggests that most of the venues surveyed were frequented by people with moderate incomes. Only 23 restaurants completely banned smoking, and seven restaurants and two bars had non-smoking areas, four of which were not completely separated from the smoking areas. In one of the 23 venues with complete smoking bans and in five of the nine venues with partial smoking bans, smoking occurred during sampling, and in only one venue was there an intervention to stop the smoking.
Characteristics of hospitality venues surveyed in five cities during July to September 2007
Although there were numerically more restaurants with smoking bans in Beijing and Xi'an than the other cities, a Fisher exact test showed that there was no statistically significant overall difference across the five cities in the proportions of venues with no smoking regulations (χ2 (8)=10.12, p=0.199).
Table 2 presents the data collected from the 404 hospitality venues, which includes active smoking behaviours observed during sampling and geometric means of both outdoor and indoor PM2.5 levels. Smoking was observed in 77.5% (313) of the surveyed venues during sampling, and the overall average ASD of these 313 venues was 1.0 burning cigarettes per 100 m3. Pairwise comparisons showed no statistically significant differences in average ASD among five cities, while it was statistically higher in bars (1.9) than that in restaurants (0.8) (t (76.67)=3.84, p<0.001, data not shown). The outdoor and indoor PM2.5 levels were 79 and 99 μg/m3, respectively, in the 91 places without smoking observed, and they were 77 and 208 μg/m3, respectively, in the 313 smoking venues. UNIANOVA test showed that in each city, when the outdoor PM2.5 levels were controlled as a covariate, the indoor PM2.5 levels of venues with active smoking observed were consistently significantly higher than those of venues without smoking observed (F=80.49, p<0.001).
Observation of cigarette smoking and PM2.5 level (μg/m3) in restaurants and bars in five cities in China, July to September 2007
Table 3 shows the PM2.5 levels in venues stratified by smoking bans and cities. Paired-sample Student t test indicated that there was a significant statistical difference between indoor and outdoor PM2.5 levels (t(403) =19.95, p<0.001). When stratified by whether smoking was observed or not, outdoor PM2.5 levels were all lower than corresponding indoor PM2.5 levels even in venues without smoking observed (table 2), but for venues with complete smoking bans, outdoor PM2.5 levels were all higher than corresponding indoor PM2.5 levels (table 3). This indicated that though there was no observed smoking during sampling in some venues allowing smoking, smoking might have happened before sampling or might have been missed by surveyors during observation; thus, some PM2.5 might be produced and kept inside the venue, leading to higher indoor PM2.5 levels than outdoors.
Geometric mean outdoor and indoor PM2.5 levels (μg/m3) in venues with different smoking policies
Table 4 shows the Spearman and partial correlation analysis of PM2.5 levels, ASD and OD. Indoor PM2.5 levels were significantly positively correlated with the outdoor PM2.5 level (Spearman ρ=0.58, p<0.001), ASD (Spearman ρ=0.52, p<0.001) and OD (Spearman ρ=0.33, p<0.001) for bivariate Spearman correlation analysis. Partial correlation analysis also showed significant positive correlation between indoor PM2.5 levels and outdoor PM2.5 levels (partial ρ=0.37 p<0.001) and between indoor PM2.5 levels and ASD (partial ρ=0.34, p<0.001). There existed no significant correlation between indoor PM2.5 levels and OD when the outdoor level and ASD were controlled.
Correlation analysis of indoor PM2.5 level with outdoor PM2.5 level, ASD and OD
Linear regression analysis (table 5) also indicated that when other factors were adjusted, the OD and city were not significantly statistically related to the indoor PM2.5 level, while the outdoor PM2.5 level, the ASD and the type of the venues were all significantly statistically related to the indoor PM2.5 level. When the ASD was removed from the second model, the R2 decreased 16% (0.08/0.49=0.16), that is, without the predictor of the ASD, the model's potentiality to explain the variability of the indoor PM2.5 level decreased 16%, and this confirms the significant correlation between smoking and indoor PM2.5 level.
Regression models on the log value of indoor PM2.5 level and its related influential factors
Discussion
The study shows indoor PM2.5 levels are highly related to active smoking density. Places with smoking observed had much higher indoor PM2.5 levels than where no smoking was observed, while in places completely banning smoking, indoor PM2.5 levels were similar with outdoor levels. Even for venues with really high outdoor PM2.5 levels like those in Xi'an and Beijing, indoor PM2.5 levels in venues with active smoking observed were significantly higher than those in venues without smoking observed, adjusting for the outdoor PM2.5 levels. These indicate that although tobacco smoke is not the sole source of indoor PM2.5 in these venues, it is a major source.
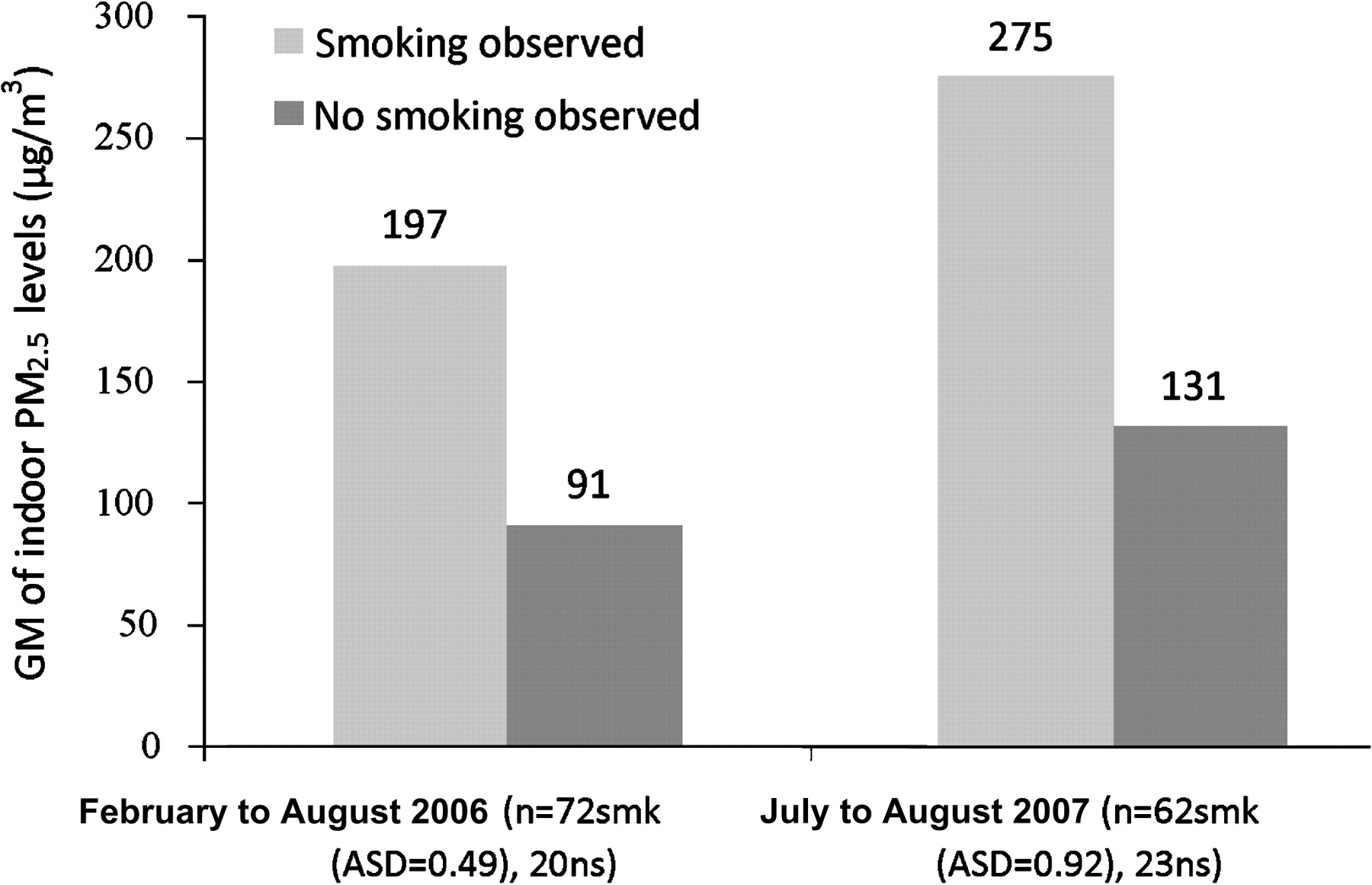
PM2.5 levels in smoking places are consistently higher than those in smoke-free places across different countries. Hyland et al5 assessed indoor PM2.5 levels in 1822 public places cross 32 countries from September 2005 to November 2006, using a standard measurement protocol which was adopted by this study. Figures 1 and 2 compare the results of that study and the present study. PM2.5 levels were measured in 92 hospitality venues in Beijing, China, in 2006, and we can see from figure 1 that indoor PM2.5 levels either in places with smoking observed or in those without smoking observed were lower than indoor levels assessed in the present study. For places without smoking observed, this might be caused by the correspondingly higher outdoor PM2.5 levels possibly due to different seasons when the two studies were conducted. Venues in Beijing in this study were sampled in July and August, 2007, while the other study was conducted from February to August, which included the Spring season with relatively lower outdoor PM2.5 levels. For places with smoking observed, the increased indoor PM2.5 level may be attributed to both the correspondingly increased outdoor PM2.5 levels and the higher ASD. Also, indoor PM2.5 levels in places with smoking observed in this study are higher than that in places with almost equal ASD in the USA, and it is also higher in places without smoking observed than that in the USA and Ireland, which has enacted national comprehensive smoke-free indoor air laws (figure 2). This probably resulted from the higher outdoor PM2.5 levels in the five cities of China.

Geometric mean (GM) of PM2.5 levels of venues in Beijing by studies. smk, smoking observed; ns, no smoking observed.

Geometric mean (GM) of indoor PM2.5 levels in China, USA and Ireland. smk, smoking observed; ns, no smoking observed.
The only effective way to protect people from SHS is creating 100% smoke-free environments by implementing smoke-free laws and legislations. As of 1 April 2008, 15 countries and 45 regions, including Hong Kong, have enacted national or local comprehensive smoke-free laws and regulations in restaurants and bars.14 However, in mainland China, smoking regulations have been limited to places like museums, libraries and waiting rooms, and only Guangzhou and Shenzhen of Guangdong Province prohibit smoking in restaurants with air conditioning.15 So, at the time of this study, hospitality venues in mainland China had smoking policies dependent on their owners. This study shows that only 23 of the 404 (5.7%) surveyed venues have smoking bans, and the indoor PM2.5 levels are very high in restaurants and bars, indicating that in mainland China, hospitality workers as well as patrons of these venues were at high risk of SHS exposure.
According to a study on hospitality patronage's attitudes towards smoke-free regulations in public places, only 30.0% and 19.8% of the patrons support completely banning smoking in restaurants or bars, respectively,16 and according to China Tobacco Control Report 2007, 52.2% of restaurant owners worry that smoking bans would reduce their revenues,17 a common belief that has been demonstrated to be false in systematic reviews of the economic impact of smoke-free laws across many jurisdictions in North America, Australia and other Western countries.18 These public opinion data as well as the observed smoking during samplings in non-smoking areas of five of the nine venues with partial smoking bans and in one of the 23 venues with complete smoking bans demonstrate that challenges exist in China to implement legislation to protect the public from SHS hazards, particularly in hospitality venues.
This study demonstrated high levels of outdoor particle air pollution in some big cities in China and also demonstrated that levels are substantially worse than outdoors in indoor environments with smoking. There is currently a great deal of discussion on reducing the very high air pollution levels in China, which lead to over 400 000 premature deaths each year, and result in total associated health costs estimated at 157 to 520 billion Yuan in 2003.19 In fact, billions of dollars were spent to improve outdoor air quality for the recent 2008 Beijing Olympic Games.20 For exposed individuals, indoor smoking represents a harmful air pollution exposure at least as bad as outdoor pollution. However, comprehensive smoke-free indoor air policies are a simple virtually cost-free solution that will dramatically reduce this exposure.
The current study measured PM2.5 exclusively, whereas other investigators have relied on nicotine measures for greater specificity to tobacco smoke exposure. PM2.5 is still an effective marker for SHS and also provides a more general air pollution measure that is effective for comparisons to other sources of pollution, such as outdoor particle levels. The laser photometer used in this study also provides continuous measurements demonstrating immediate changes in particle levels as conditions change or the device is moved between different microenvironments (figure 3).

{kind=link}
{kind=link}
{kind=link}
Real-time monitoring of PM2.5 level in a restaurant with smoking observed and in anther one without smoking observed in Beijing.
Although this study adopted a convenience sample of venues, the results of this study were able to reflect the general situation of tobacco control and SHS exposures in hospitality venues in the five cities of China, as we have taken into account different types of venues, their possible proportions, their holding capacity and average expense.
Conclusions
PM2.5 levels in places with smoking observed are significantly higher than those in smoke-free places and are statistically associated with active smoker densities. SHS exposures are very serious in hospitality venues in the five cities in China, and comprehensive smoking regulations are commonly wanted to protect the public from SHS hazards.
What this paper adds
The Framework Convention on Tobacco Control calls for the expansion of smoke-free places in signatory countries to protect people from SHS hazards. However, up until the time when this study was conducted, there were almost no smoking regulations in hospitality venues in mainland China, and quantitative assessments of SHS exposure in these venues were quite limited. This study was the largest study to assess indoor SHS exposure in hospitality venues in mainland China and so to provide scientific evidence for the Chinese government to adopt effective measures to reduce or eliminate SHS hazards in hospitality venues.
The results of this study showed that, without smoking regulations, only few (7.9%) restaurants and bars had smoking regulations and SHS exposure in these places was very high. The PM2.5 levels in venues with smoking observed was more than two times of the levels in venues without smoking observed, and only when smoking was completely banned, could the indoor PM2.5 levels become similar with corresponding outdoor levels. These results underline the importance of comprehensive smoke-free policy in accordance to Framework Convention on Tobacco Control.
For the purpose of the 2008 Olympic Games, China initiated a series of tobacco control activities in public places including hospitality venues to reduce SHS exposure; this study could provide baseline information for further studies aimed to evaluate the effectiveness of the tobacco control activities in hospitality venues.
Acknowledgments
The authors would like to acknowledge the Chinese National Center for Disease Control and Prevention (CDC) and the local CDC or health institutions representatives in each city for their role in data collection.
Footnotes
Funding This project was supported by a special grant from the Chinese National Center for Disease Control and Prevention on Framework Convention on Tobacco Control annual implementation for 2007 and by a grant from the Roswell Park Trans-disciplinary Tobacco Use Research Center (P50 CA111236). MJT was supported by a grant from the Flight Attendant Medical Research Institute. The funding sources had no role in the study design, in collection, analysis and interpretation of data, in the writing of the report, and in the decision to submit the paper for publication.
Competing interests None.
Ethics approval This study was approved by the Ethics Review Board Committee of Chinese National Center for Disease Control and Prevention.
Provenance and peer review Not commissioned; externally peer reviewed.