Article Text

Abstract
Objective To better understand the current embrace of long-term nicotine maintenance by British governmental agencies and tobacco harm reduction by several leading British public health organisations, describe the context and deliberations of the UK’s first formal tobacco risk reduction programme: ‘Product Modification’.
Methods Analysis of previously secret tobacco industry documents, news archives and Parliamentary debate records.
Results From 1972 to 1991, the British government sought to investigate safer smoking through the ‘product modification programme'. The Independent Scientific Committee on Smoking and Health (ISCSH) advised the British government on these efforts and collaborated with the tobacco industry, with which government then negotiated to determine policy. The ISCSH operated from four industry-backed premises, which contributed to the ISCSH’s support of safer smoking: (1) reduced toxicity indicates reduced risk; (2) collaboration with the tobacco industry will not undermine tobacco control; (3) nicotine addiction is unavoidable; (4) to curtail cigarette use, solutions must be consumer-approved (ie, profitable). These premises often undermined tobacco control efforts and placed the ISCSH at odds with broader currents in public health. The product modification programme was abandoned in 1991 as the European Community began requiring members to adopt upper tar limits, rendering the ISCSH redundant.
Policy implications Endorsements of reduced harm tobacco products share the same four premises that supported the product modification programme. Current tobacco harm reduction premises and policies supported by the British government and leading British public health organisations may reflect the historical influence of the tobacco industry.
- tobacco industry
- tobacco industry documents
- public policy
- harm reduction
Statistics from Altmetric.com
Introduction
Tobacco harm reduction has increasing prominence in scientific and policy discussions.1 The British Medicines and Healthcare Products Regulatory Agency endorsed long-term nicotine use in 2009,2 approved classifying pre-approved electronic cigarettes (e-cigarettes) as medicines in 20133 and has licensed two such products as medicines, although these have yet to come to market.4 The UK is one of 20 countries worldwide that classifies certain e-cigarettes as medicinal.5 Major British public health organisations support tobacco harm reduction for smokers struggling to quit.1 6 7 The USA, in contrast, classifies e-cigarettes as tobacco products and leaders are less supportive of tobacco harm reduction.8
Historians have attributed this transatlanticdifference to the tobacco industry’s long history of deception over ‘safer’ products resulting in scepticism towards tobacco harm reduction.8–10 Green et al locate the divergence of opinion in differing experiences with harm reduction more broadly.11 In the UK, the Ministry of Health embraced drug harm reduction as early as the 1920s, including treatment with low doses of drugs.11 In the USA, public health policies have been more ‘prohibitionist’, with ‘tight narcotic regulation and refusal to provide narcotics to addicts as treatment or maintenance defin(ing) the US posture for decades’.11 In addition, during the 1990s, contentious consumer lawsuits played key roles in advancing US public health,12 whereas British courts saw fewer and less successful lawsuits.13
However, little has been written connecting the UK’s embrace of tobacco harm reduction to the country’s previous tobacco risk reduction efforts. Historian Virginia Berridge contextualises the current debate in these earlier failed attempts to make cigarettes safer,14 in which an expert committee—‘a distinctive British configuration’—played a key role.15 The clearest historical example of the promotion of ‘safer’ tobacco products in the UK was the ‘product modification programme,' which the British government pursued in the 1970s and 1980s, guided mainly by the Independent Scientific Committee on Smoking and Health (ISCSH).16
The goal of product modification was to create a safer cigarette, initially by substituting other materials for tobacco, and later by gradually lowering cigarettes’ tar and nicotine levels.16 The ISCSH was the chief advisory body and a ‘key site of interchange’ between government and the industry, in which ‘policy objectives and agendas defined what was legitimate and illegitimate science, and vice versa’ for years to come.15 Historians have also recognised the tobacco industry’s critical but ‘invisible’ role in mediating British smoking policy.17
To shine a light on the ‘invisible’, this paper analyses private exchanges between the ISCSH and the tobacco industry during the product odification programme. The main research questions were, ‘what was the relationship between the tobacco industry and the UK government in early tobacco risk reduction programmes, and what core premises about tobacco and harm reduction did the industry promote in these programmes?’
Methods
We analysed previously secret internal tobacco industry documents available through the Truth (formerly Legacy) Tobacco Industry Document Library (https://industrydocuments.library.ucsf.edu/tobacco/) between January 2016 and October 2017, combining historical analytical qualitative methods with iterative search strategies.18–20 Keyword searches included ‘Independent Scientific Committee on Smoking and Health’; ‘ISC’; ‘ISCSH’ and ‘Froggatt committee’; ‘Robert Hunter’; ‘Froggatt’ and ‘TAC’. Using standard snowball sampling techniques, we refined searches for key individuals and programme, and examined documents with adjacent reference (Bates) numbers and dates. This analysis is based on 203 tobacco industry documents. To contextualise this material, we triangulated with online search engines, records of Parliamentary debates, news archives and existing historiography covering British smoking history from the 1950s to 1990s to compare the rationale behind the ISCSH’s recommendations with broader national public health currents.
Results
Context
From the 1970s to 1990s, the British government involved the tobacco industry in a series of voluntary agreements regulating advertising, warning labels and cigarettes’ tar and nicotine yields.15 21 In exchange for its first 1971 agreement, government agreed to not introduce harsher legislative controls on tobacco for several years.22 The tobacco industry policed these voluntary agreements itself, and violations—of which there were 462 by 198823—rarely resulted in penalties.24 25 These agreements characterised British tobacco control polices for the duration of the ISCSH’s tenure.
Although inappropriate by today’s standards,26 these agreements both upheld a British tradition of seeking solutions through consensus with industry15 27 and reconciled the government’s duty to promote public health with its economic dependence on tobacco taxes.15 21 28 Failure to enact policies mandating smoke-free workplaces in the 1980s was attributed to this dependence.29 30
Scientific opinion through the early 1970s understood low-tar cigarettes as safer alternatives to high-tar cigarettes.15 Government and industry established a scientific liaison committee in 1971 to investigate product modification (ie, the creation of a safer cigarette).31 The Standing Scientific Liaison Committee (SSLC) began work in 1972. In 1973, following the SSLC’s first and only report,32 the Department of Health began publishing the tar and nicotine yields of all cigarettes sold in the UK, facilitating switching to lower tar and nicotine brands.32
In 1973, the ISCSH replaced the SSLC. The Department of Health and Social Services (DHSS) appointed the ISCSH’s members—all but one—unpaid, prominent academics.33 The 1960s Committee on the Safety of Medicines (CSD) provided the structural template (and eventually several personnel) for the ISCSH.34 Robert Hunter, renowned physician and vice chancellor at the University of Birmingham, and prior CSD clinical trials subcommittee Chair, served as the ISCSH’s first Chairman from 1973 to 1981. Peter Froggatt, vice chancellor of the Queen’s University, replaced Hunter as Chairman, serving from 1982 to 1991.
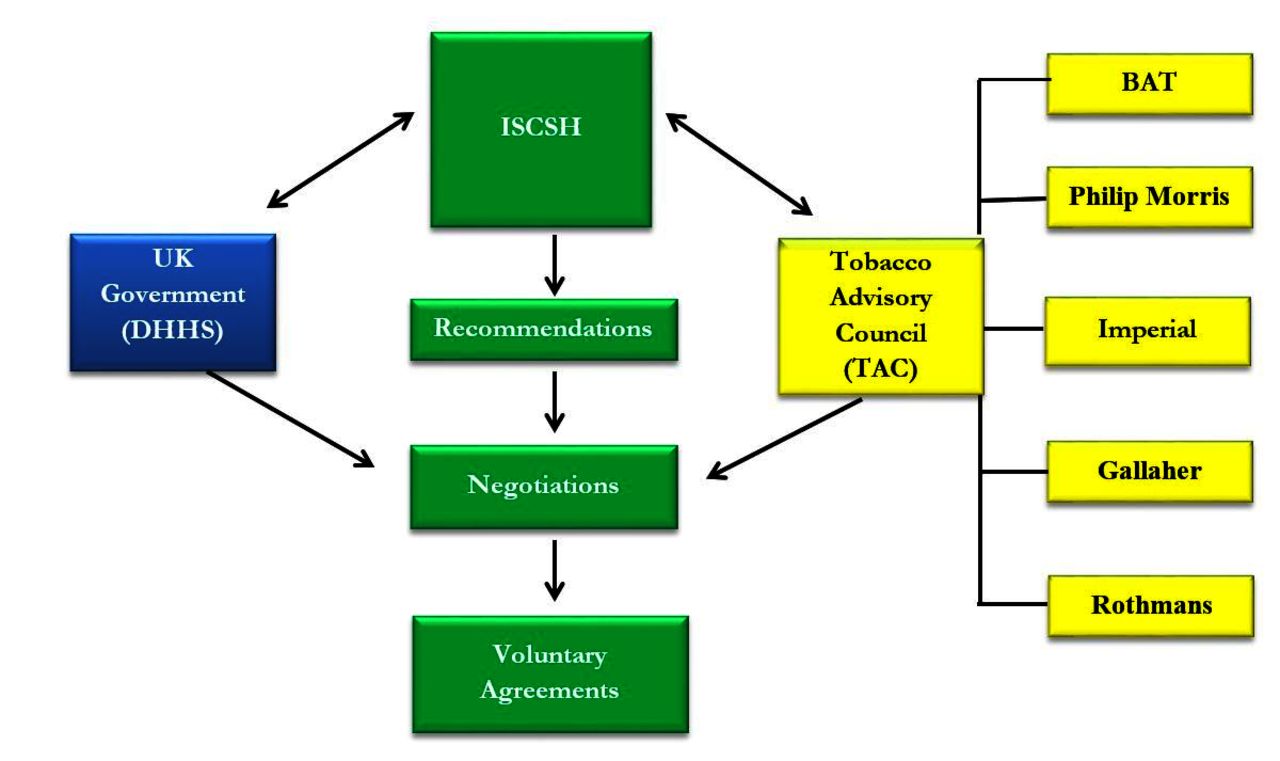
From 1973 to 1991, the ISCSH was the government’s chief advisory body on smoking and health.15 While government appointed its members, the ISCSH was required to consult with and depended on research from the British tobacco industry’s chief trade and lobbying group, the Tobacco Advisory Council (TAC)— itself made up of representatives from every major tobacco company in Britain. The ISCSH then made recommendations to the DHSS. These recommendations served as the basis for negotiations between government and the tobacco industry to determine future voluntary agreements (figure 1).15–17

{kind=link}
The UK Department of Health and Social Services (DHSS) appointed Independent Scientific Committee on Smoking and Health (ISCSH) members. The ISCSH then made recommendations back to the Department of Health, which in turn served as the basis of future negotiations between industry (Tobacco Advisory Council (TAC)) and government to determine tobacco control policies. Through the TAC, representatives of each of the major British tobacco companies gave feedback, criticism and research to the ISCSH, thereby influencing the Committee’s recommendations to the DHSS. Voluntary agreements between the TAC and the British government would help determine national tobacco policy through the 1990s. Blue, public health; yellow, tobacco industry; green, industry-influenced group and activities. BAT, British American Tobacco.
The ISCSH drafted four reports—(in 1975, 1979, 1983 and 1988)—setting guidelines for testing tobacco substitutes, detailing tar-yield reduction targets, and assessing quality of evidence on smoker compensation and second-hand tobacco smoke.33 35–37 Online supplemental table 1 compares the product modification programme and positions of government, industry and public health opinion over time.
Supplementary file 1
ISCSH premises
The ISCSH’s tenure spanned several ideological shifts in British public health.13 In the early 1970s, industry and public health interests aligned—although for different reasons—to develop a ‘safer cigarette’, first using tobacco substitutes. The unpopularity of these products, coupled with the discovery of compensation divided the industry and major British public health organisations for subsequent decades.34 However, government continued collaboration with the industry via the ISCSH to lower tar and nicotine yields. Conversely, by the late 1970s public health groups advocated for the elimination of smoking rather than its modification.13 Health concerns about passive smoking further diminished future collaborations between public health and the tobacco industry,17 but government continued industry partnership and voluntary agreements through the mid-1990s.15
Throughout these shifts, four main premises appear to have consistently guided the ISCSH’s work and recommendations. These premises were predicated on an early 1970s evidence base, and a norm of scientific and financial dependence on the tobacco industry. Each premise generated policy recommendations beneficial to the tobacco industry and detrimental to public health. These premises enabled the promotion of product modification for a decade longer than British public health organisations outside the ISCSH.
Reduced product toxicity indicates reduced risk
The ISCSH’s first attempt to promote ‘safer smoking’ was to approve new cigarettes with one-quarter of the tobacco replaced with a tobacco substitute. The ISCSH approved modified cellulose cigarettes in their first report issued in 1975.12 33 The products nonetheless failed to attract customers.38 Had these products succeeded, the fate of the ISCSH may have been different. Virginia Berridge notes that the Minister of Health from 1974 to 1976, David Owen, hoped to use the success of tobacco substitutes to regulate tobacco under provisions of the 1968 Medicines Act.13 34 In January 1976, Owen’s MP-ally Robert Kilroy-Silk proposed controlling tobacco products as medicines and upgrading the ISCSH into a regulatory committee.28 The strategy was abandoned following the failure of tobacco substitutes, opposition from fellow MPs and Owen’s reassignment to the Foreign Office.34
The second decade of the ‘product modification programme' centred on lowering tar yields (and presumably toxicity) in cigarettes. This approach assumed that the most toxic materials are in the tobacco tar (which was correct), and that smokers would not ‘oversmoke’ cigarettes with lower tar yields (which was not).38 Smokers’ compensation later revealed that low-tar cigarettes were sometimes even more dangerous than high-tar cigarettes.39 40
Aware of compensation since at least the mid-1970s,41 the industry worried that compensation could ‘undermine consumers’ confidence in the ISCSH’s efforts to reduce tar levels and thereby ‘imperil the achievement of tar reduction objectives in the current Voluntary Agreement’.42 In 1981, the Chairman of the Tobacco Advisory Council (TAC), James Wilson, asked the ISCSH in one of their many private meetings, to ‘reaffirm to (the British government) and (the) TAC their (ie, the ISCSH’s) continuing belief in the principle of tar reduction’.42 Peter Froggatt, then Chairman of the ISCSH, countered that smokers’ compensation might undermine the product modification programme.43 The TAC insisted ‘there is little evidence of full compensation’ and urged the ISCSH not ‘exaggerate directly or indirectly (its) significance’.44
According to internal documents that were not shared with the ISCSH, the industry had significant financial and political dependence on the low-tar programme. In an August 1983 letter to BAT’s board of directors, Lionel Blackman, BAT’s Director of Research and Development for Europe, stated the ‘strong worldwide move towards claiming that people compensate completely and, therefore, that the low tar program is a fraud’ represented ‘the toughest challenge yet to the maintenance of industry credibility’.45 Blackman believed discrediting low tar would lead to dissolution of the ISCSH and far more stringent industry regulation.45 He encouraged accepting reducing tar to 13 mg by 1987 rather than the UK government’s ‘logical alternative’ of tax increases, which would drive away far more consumers.45 It was of ‘over-riding importance’ not to alienate Froggatt and the ISCSH, maintain voluntary agreements and ‘to get Government to acknowledge its support of the low tar concept’.45 Consistent with the TAC’s requests, the ISCSH’s 1983 report stated that there was ‘no clear evidence of marked compensation over long periods’ and while ‘some (compensation) may occur…the lowering of tar and nicotine yields would still result in reduced average intake of these substances’.46
In 1988, consistent with the US Surgeon General’s Report,47 the ISCSH final report stated that reducing tar yields might not render cigarettes ‘safer’.37 The ISCSH nonetheless supported ‘the lower-yield approach as one part of a general strategy aimed at reducing the extent of disease caused by smoking, while at the same time making the public aware of the limitations of that approach’.37
Collaboration with the tobacco industry will not undermine tobacco control efforts
In the late 1970s, the discovery of compensation prompted prominent physicians and grass-root organisations, most notably, Action on Smoking and Health (ASH) to de-emphasise risk reduction (eg, safer smoking) and promote cessation and prevention.15 31 34 Whereas product modification required the industry’s collaboration with government, a focus on prevention and cessation did not need cooperation with tobacco companies. In 1976, the DHSS issued a booklet supporting prevention and cessation, although it also stated controls should only be introduced ‘after consultation with interests likely to be substantially affected'.48 Based on evidence of compensation, the Health Education Council, a government-funded charity, likened safer smoking to ‘jumping from the 36th floor of a building instead of the 39th'.17 ASH simultaneously called for more taxation, media campaigns, advertising bans and ending government partnership with the tobacco industry.15 34 49
In 1977, Robert Hunter, the ISCSH’s first chairman, gave a speech to a joint conference of the British and Scottish Thoracic Societies in which he defended the industry and the ISCSH’s partnership and focus on risk reduction. To Hunter, industry support of tobacco substitutes and low-tar cigarettes was necessary to get consumers to switch.50 By extension, any policy that antagonised the industry or that threatened its profits would foreclose the real possibility of a safer cigarette, which, he argued, the industry alone had the expertise and incentive to produce.50
On several occasions, industry partnership weakened the ISCSH statements on tobacco risks and delayed policy action. For example, in 1978, on seeing a draft of the ISCSH’s second report, HB Grice, then chairman of the TAC, asked that the ‘scientifically inappropriate’ word ‘addictive’ be replaced with the more correct and less emotive ‘dependence inducing’.51 The final draft did not use the word addictive.35 The TAC also asked that the report mention the industry’s ‘impressive progress’ in reducing tar yields up until that point,51 despite concerns expressed in the broader scientific community, several ISCSH members—and, privately, the industry—about whether compensation negated any benefit from tar reduction.38 The Committee obliged.35
In 1981, several studies demonstrated a dose-response relationship between exposure to smoke and the development of lung cancer in non-smokers.52 The TAC claimed the evidence remained equivocal and that the issue was beyond the Committee’s terms of reference.53 Nonetheless, in a draft of its third report, the Committee wrote of pulmonary harms to children exposed to tobacco smoke. The TAC criticised the draft for ‘overlook(ing)…other differences besides exposure to tobacco smoke that may be significance for the observed increase of respiratory illness’ and deemed the papers showing harms of passive smoking to be ‘of poor quality’ which ‘brought science generally into disrepute’.54
In its third report, the ISCSH held its position that second-hand smoke harmed children and adults with respiratory problems, but conceded that ‘many of the reported associations, including that between passive smoking and lung cancer, have not been established unequivocally’.36 Four years later, over TAC objections, the ISCSH stated exposure to second-hand smoke increased by ‘between 10% and 30%’ the development of lung cancer in non-smokers.55
The industry’s influence on British public health extended through the 1990s through the Tobacco Products Research Trust (TPRT): an industry-funded charity established by voluntary agreement in 1982. In the late 1970s, the ISCSH had requested funds from the TAC to commission and monitor the health outcomes of product modification.56 Ultimately, the TAC gave the TPRT £1 million a year for 3 years.34 By 1987, the Trust funded 60% of all research on smoking conducted in Britain, yet conducted no experiments on smoking cessation or prevention.57
In a book summarising the Trust’s work, Peter Froggatt, chairman of the Trust, emphasised the importance of industry involvement, stating that without tobacco industry funds there would have been ‘no research programme and no Trust!’ insisting that the TPRT worked independently at ‘arms-length’ from the industry.57 However, an internal planning document shows that AM Reid—a lawyer for Imperial Tobacco—told ISCSH Chairman Hunter that the TAC was happy to finance TPRT’s research, provided the industry ‘receive(d) proper assurances of support and encouragement from Ministers and officials, and an indication that the results would not be sabotaged by anti-smoking zealots’.58 Bero notes that because of industry involvement, TPRT-funded epidemiological studies (on compensation, nicotine and the adverse effects of tar) lagged far behind internal research the tobacco industry had conducted on low-tar cigarettes.56 Throughout the 1980s, several MPs criticised voluntary agreements as ineffective,59–62 but support from the government continued.63 64
Nicotine addiction is inevitable and so tobacco control solutions must include ongoing nicotine addiction
In each of its four reports, the ISCSH recommended that smokers quit, and that non-smokers not start smoking. Yet, in its 1979 report, the ISCSH wrote that because some people will nonetheless smoke, ‘it is important that such people should be enabled and encouraged to smoke less harmfully’.35 Chairman Hunter made the same argument in his 1977 speech to the British and Scottish Thoracic Societies, ‘the practical way of diminishing the risk is to produce smoking material which is less damaging and perhaps less addictive’.50
This position was at odds with the British public health community. ISCSH member Dr J Donald Ball also disagreed, submitting a minority report to the ISCSH’s second report in which he disavowed safer smoking.17 Ball argued that the only adequate responses to the epidemic ‘was preventative…requir(ing) measure which stop people smoking or prevent them starting’.65 Robert Hunter later privately apologised to the industry for the minority report ‘not only because of its philosophy but also because it detracted from the main document’.66 TAC Chairman Wilson stated that ‘anything that could be done by the (ISCSH) or the Department of Health to disclaim the minority report would be helpful; (as its) recommendations…would be picked up by anti-smokers and used in an irresponsible and damaging way’.66
The ISCSH’s 1983 Report concluded that low tar, high nicotine cigarettes should be made available to the public, while characterising compensation as a short-term phenomenon less important than lowering tar levels.36 Historian Virginia Berridge argues the growing understanding of nicotine addiction, including the TPRT’s work on nicotine and low tar, ultimately changed the ISCSH’s views on compensation, although a decade after others in British public health.34 Acknowledging compensation, the ISCSH faced a quandary: should the Committee recommend nicotine levels stay the same to prevent compensation but maintain cigarettes’ addictiveness? Or forgo worries of compensation and lower nicotine levels to wean smokers off cigarettes and prevent dependence?67
While the Committee never answered the question, compensation came to inform Froggatt’s private scepticism about the product modification programme. During a 1989 speech to the Royal College of Physicians, Froggatt agreed with critiques that the programme allowed manufacturers to continue to sell ‘zillions of cigarettes’ and conduct ‘consumer acceptability research, which can be commercially very profitable’.68 Froggatt also acknowledged that ‘tinkering with the tar/nicotine ratio’ was ‘hardly morally very edifying and only Jesuitically justifiable’.68 However, this scepticism had minimal impact.
To curtail cigarette use, solutions must be consumer-approved (ie, profitable)
After 1977, the ISCSH was allowed to make recommendations to the TAC,13 and pushed the industry to lower tar yields. However, the TAC argued that tar yields were of a ‘commercial nature’ and beyond the purview of the ISCSH.69 Despite agreeing to tar and nicotine reductions, the industry fought for profitable targets. For example, the Committee met with the TAC to discuss the product modification programme’s shift away from substitutes towards low-tar cigarettes. Here, Chairman Hunter suggested a tar ceiling of 10 mg within the next few years, to which the industry’s response was, according to the anonymous author of the TAC’s meeting notes, ‘extremely uncooperative, if not hostile’.70 The ISCSH’s second report committed to an average tar yield of 15 mg/cigarette within 4 years.
In 1978, the TAC argued that the ISCSH’s recommended tar reductions should depend on consumer demand.51 In June 1979, the TAC then argued, ‘the rate and timing of any (future) reductions’ were ‘primarily political and commercial, and not scientific’ and thus the industry argued the ISCSH was unqualified to make such recommendations.66 The ISCSH was not alone in assuming public health and industry profit must be aligned. In proposing to bring the ISCSH under the Medicines Act, David Kilroy-Silk MP, stated that ‘the industry would be fully involved and consulted at all stages’ of the move.28 In 1980, one Conservative MP voiced support for product modification precisely because it conveniently ‘allow(ed) smokers to have the benefits which they derive from smoking, the Chancellor to have the revenue from the tobacco tax, (and) the tobacco worker[s]…up and down the country to retain their jobs’.71
Tobacco companies successfully delayed the introduction of lower tar products that it thought would be unpopular with consumers, while simultaneously arguing they would improve smokers’ health in a manner ‘consistent both with the need to reduce the harmful effects on health of smoking and with commercial practicalities’.35 The ISCSH continued promoting product modification until the Committee’s end in 1991. To one embittered MP, product modification had ultimately represented an attempt to ‘serve two masters—highlighting the health hazards associated with tobacco while also making use of the revenue it produced’.72 The government terminated the ISCSH in anticipation of 1992 European Community regulations requiring members to establish upper tar levels in cigarettes, rendering the ISCSH redundant.34
Discussion
This study demonstrates that partnership with, and reliance on industry advice and research previously led to significant delays in the implementation of more comprehensive tobacco control measures in the UK. The tobacco industry stalled public health progress by influencing the ISCSH’s beliefs about compensation, the dangers of low-tar cigarettes, the neutrality of industry-financed research and, to a lesser degree, the dangers of passive smoking.
Through the late 1980s, the ISCSH continued to work under four premises established in the early 1970s, when industry and public health interests were briefly aligned. However, as major British public health organisations in the UK changed, the ISCSH remained wedded—by government mandate—to an outdated evidence base and tobacco industry influence. This led to the promotion of ‘safer smoking’ for a decade beyond the rest of the British public health community, and supported weak voluntary agreements as alternatives to stronger measures.73
Government and industry collaborations to develop a ‘safer cigarette’ were not unique to the UK. From 1968 to 1979, the US National Cancer Institute spent US$50 million to sponsor the Tobacco Working Group (TWG). Industry representatives in the TWG withheld relevant information from fellow Group members, disputed findings they knew to be true and lobbied against funding for research on prevention and pharmacological interventions for smoking cessation.12 The TWG’s funding ended in 1979 in favour of prevention and cessation,74 while the ISCSH continued to work alongside the industry for another 12 years.
In the eyes of the broader British public health community, the ISCSH work was largely for naught. Yet in recent years, the Committee’s guiding logic and premises of risk reduction have enjoyed a reanimation among British public health organisations.34 Through the 1990s, ‘safer’ tobacco products were put forward for smokers who failed pharmacotherapy.34 The term ‘tobacco harm reduction’ stated in an Institute of Medicine 2001 report, which purposely avoided the term ‘safer cigarette’ to avoid implying that any tobacco product is ‘safe’.75 ‘Tobacco harm reduction’ has since come primarily to denote long-term nicotine maintenance with ‘safer’ products.
Berridge characterises this new ideology of smoking treatment as ‘pharmaceutical public health’.13 15 As tobacco companies begin to offer products that appear increasingly like pharmaceuticals, they also recast themselves as a public health partners.76 Since 2009, tobacco companies have started promoting e-cigarettes and resurrecting ‘heat-not-burn’ cigarettes, arguing that such products are safer than cigarettes.77
The prospect of an industry-public health alliance has similarly re-emerged. In 2016, the British government licensed two British American Tobacco products as medicines,4 and in October 2017, Philip Morris International (PMI) began seeking public health partnerships for its Foundation for a Smoke-Free World.78 As with the TPRT, PMI insists it will have an arms-length relationship with the research of the Foundation, to which it has dedicated US$1 billion over 12 years. Despite broader scepticism in the UK,79 The Lancet recommended that public health ‘be open to dialogue and debate’ with the Foundation.80
British public health should mind past experience, in which industry-backed ‘safer cigarettes’ undermined public health. The same four premises that guided the ISCSH to their detriment and protected the UK tobacco industry continue to feature prominently in the current British embrace of tobacco harm reduction (see online supplemental table 2). This raises the question of whether the new products are indeed ‘revolutionary’, or constitute another iteration of the ‘safer cigarette’ that functions principally to delay more comprehensive regulations, bolster declining markets, attract new users and improve the industry’s public image.81
While the ISCSH’s premises did not clearly originate from the tobacco industry itself, the industry has long aggressively promoted them because their interests are well-represented therein. If the past is any guide, the promotion of tobacco harm reduction may serve the interests of tobacco companies more effectively than the public. Regulatory bodies should consider toxin exposure, and new products’ actual use, abuse potential and population health effects before endorsing them as safer.10
What this paper adds
The British government endorses long-term nicotine replacement therapy and most major British public health organisations endorse tobacco harm reduction.
The UK’s current embrace of tobacco harm reduction has a specific historical context that warrants examination. To this end, this paper examines the context of and relationship between the tobacco industry and the British government during country’s first formal tobacco harm reduction programme: the ’product modification programme' of the 1970s and 1980s.
This paper looks specifically at the core premises about tobacco and harm reduction that the industry promoted during the ‘product modification programme.' These assumptions benefited the tobacco industry and undermined public health. Under industry influence, the ISCSH’s positions often lagged behind the rest of the public health community. British public health authorities are again using these four guiding premises in current tobacco harm reduction positions and policy, which may unwittingly reflect the historical influence of the tobacco industry.
References
Footnotes
Contributors JE acquired the data for this study and led the analysis, drafting and writing. PML obtained funding, supervised data collection, analysis and performed critical revisions. Both authors jointly conceived the study, contributed to data analysis, writing and revision and approved the final version of the article for publication.
Funding This work was supported by the National Cancer Institute at the National Institutes of Health under award number R01-CA-87472.
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This paper is an analysis of previously secret tobacco industry documents. The data are freely available to the public at the UCSF Truth Industry Documents Library. https://www.industrydocumentslibrary.ucsf.edu/